种植牙修复前后脱氧吡啶啉和C-反应蛋白的变化
2017-06-05 14:20李钟鹏韦惠平陈华韦启升
中国现代医学杂志 2017年9期
李钟鹏,韦惠平,陈华,韦启升
(1.广西医科大学附属口腔医院 综合一门诊 广西 南宁 530021;2.广西壮族自治区人民医院口腔科,广西 南宁530021;3.广西壮族自治区桂林市口腔医院,广西 桂林 541001)
种植牙修复前后脱氧吡啶啉和C-反应蛋白的变化
李钟鹏1,韦惠平2,陈华3,韦启升3
(1.广西医科大学附属口腔医院 综合一门诊 广西 南宁 530021;2.广西壮族自治区人民医院口腔科,广西 南宁530021;3.广西壮族自治区桂林市口腔医院,广西 桂林 541001)
目的探讨人工种植牙修复患者手术前后尿脱氧吡啶啉和血清C-反应蛋白的变化。方法选取2011年7月-2016年6月广西区内种植体周围炎患者60例作为种植体周围炎组,健康种植体患者60例作为健康种植体组,健康体检者60例作为对照组。测定尿脱氧吡啶啉含量和血清C-反应蛋白水平。结果3组术前尿脱氧吡啶啉含量和血清C-反应蛋白水平比较,差异无统计学意义(P<0.05);种植体周围炎组术后尿脱氧吡啶啉含量和血清C-反应蛋白水平均高于术前及对照组(P<0.05);健康种植体组术后1个月尿脱氧吡啶啉含量和血清C-反应蛋白水平均高于术前及对照组(P<0.05);术后1个月,种植体周围炎组患者尿脱氧吡啶啉含量和血清C-反应蛋白水平均高于健康种植体组(P<0.05);种植体周围炎组和健康种植体组患者血清C-反应蛋白水平与尿脱氧吡啶啉含量均呈正相关(P<0.05)。结论人工种植牙修复术后发生种植体周围炎时,尿脱氧吡啶啉和血清C-反应蛋白水平升高,人工种植牙修复术后健康种植体患者尿脱氧吡啶啉和血清C-反应蛋白水平也升高。
口腔种植修复;种植体周围炎;尿脱氧吡啶啉;C-反应蛋白
随着生活水平的提高、人们观念的转变及人工种植牙技术的不断发展,种植修复理念已被广泛接受,一些个体诊所和基层医院也掌握人工种植牙技术。随着人工种植牙技术的普及,种植体周围病变的发生率不断增加,种植体周围病变比较复杂,目前缺乏有意义的实验室诊断标准。尿脱氧吡啶啉可以特异性反应骨的改建和吸收[1-3],C-反应蛋白是常用的高度灵敏的急慢性炎症筛查指标,与牙周病变也有明显的相关性[4-6]。种植体周围病变的发生、发展过程除伴有细菌感染引起的炎症反应,还伴有牙槽骨的转化吸收。本文对人工种植牙修复患者手术前后尿脱氧吡啶啉和血清C-反应蛋白的变化进行研究。
1 资料与方法
1.1 临床资料
选取2011年7月-2016年6月广西区内种植体周围炎患者作为种植体周围炎组,健康种植体患者作为健康种植体组、健康体检者作为对照组,每组60例。目前种植体周围炎的诊断尚无统一标准,本研究结合临床表现和辅助检查,采用以下指标进行诊断:没有典型疼痛;黏膜肿胀充血;轻柔探诊后有出血;种植体周围袋探诊深度≥5 mm;曲面断层片提示牙槽嵴顶骨有吸收。本研究经广西医科大学附属口腔医院伦理委员会审批,所有研究对象签署知情同意书。
纳入标准:种植体修复治疗患者均接受口腔单颗种植体修复治疗;种植体周围炎为种植修复术后1个月内诊断为种植体周围炎患者;所有患者均自愿参与研究,资料完整。
排除标准:患骨质疏松、糖尿病、甲状腺功能亢进症、冠状动脉粥样硬化性心脏病、肝肾功能损害、恶性肿瘤等全身系统性疾病者;3年内有吸烟史者;存在牙周组织病变者;近3个月内服用糖皮质激素、免疫制剂、消炎药物者;3个月内服用过避孕药者;绝经期、妊娠期及哺乳期女性。
1.2 研究方法
1.2.1 标本采集 种植体周围炎组和健康种植体组患者收集种植体修复前和种植体修复术后1个月时的标本,对照组收集体检当天的标本。血液采集外周静脉血送检,留取血清进行血清C-反应蛋白检测;尿液采集:嘱患者禁食、禁水10 h后,留取中断清洁尿50 ml送检。
1.2.2 尿脱氧吡啶啉含量测定 取10 ml尿液于离心管中,1 500 r/min离心5 min,取上清液采用化学发光分析仪测定尿脱氧吡啶啉,并采用全自动生化分析仪测定尿肌酐,为矫正尿液浓缩引起的误差,尿脱氧吡啶啉含量以尿脱氧吡啶啉/尿肌酐表示。
1.2.3 血清C-反应蛋白测定 采用全自动蛋白分析仪测定血清C-反应蛋白浓度。
1.3 统计学方法
数据分析采用SPSS 20.0统计软件,计量资料以均数±标准差(±s)表示,用t检验或方差分析,两两比较用LSD-t法,计数资料以率(%)表示,用χ2检验,相关分析用Pearson法,P<0.05为差异有统计学意义。
2 结果
2.1 一般资料
3组患者年龄、性别比较,差异无统计学意义(P> 0.05),见表1。
2.2 3组患者术前尿脱氧吡啶啉和血清C-反应蛋白水平比较
种植体周围炎组、健康种植体组和对照组术前尿脱氧吡啶啉含量和血清C-反应蛋白水平比较,经方差分析,差异无统计学意义(P<0.05)。见表2。

表1 3组患者一般资料比较 (n=60)
表2 3组患者术前尿脱氧吡啶啉含量和血清C-反应蛋白水平比较 (n=60,mg/L,±s)
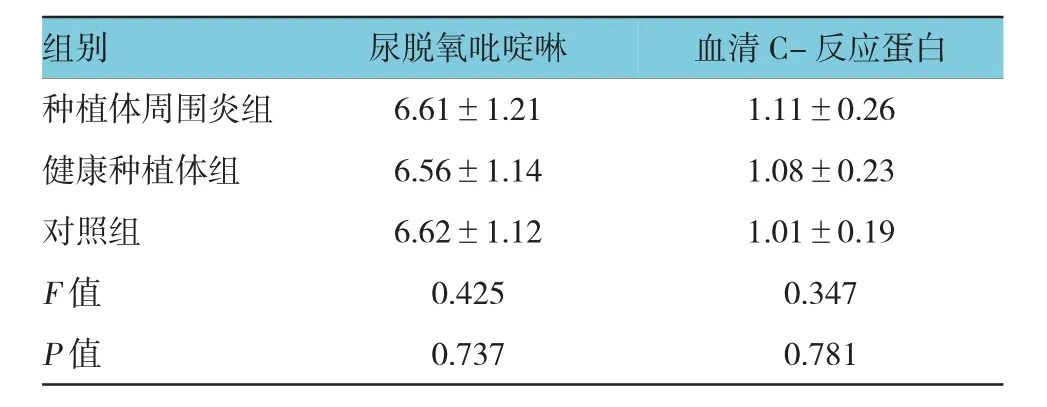
表2 3组患者术前尿脱氧吡啶啉含量和血清C-反应蛋白水平比较 (n=60,mg/L,±s)
组别 血清C-反应蛋白种植体周围炎组 6.61±1.21 1.11±0.26健康种植体组 6.56±1.14 1.08±0.23对照组 6.62±1.12 1.01±0.19 F值 0.425 0.347 P值 0.737 0.781尿脱氧吡啶啉
2.3 种植体周围炎组与对照组的尿脱氧吡啶啉含量和血清C-反应蛋白水平比较
种植体周围炎组术前、术后1个月及对照组的尿脱氧吡啶啉含量和血清C-反应蛋白水平比较,经方差分析,差异有统计学意义(P<0.05),种植体周围炎组术后尿脱氧吡啶啉含量和血清C-反应蛋白水平均高于术前和对照组。见表3。
2.4 健康种植体组与对照组的尿脱氧吡啶啉含量和血清C-反应蛋白水平比较
健康种植体组术前、术后1个月及对照组的尿脱氧吡啶啉含量和血清C-反应蛋白水平比较,经方差分析,差异有统计学意义(P<0.05),健康种植体组术后1个月尿脱氧吡啶啉含量和血清C-反应蛋白水平均高于术前及对照组。见表4。
2.5 种植体周围炎组与健康种植体组患者术后1个月尿脱氧吡啶啉含量和血清C-反应蛋白水平比较
术后1个月,种植体周围炎组与健康种植体组患者尿脱氧吡啶啉含量和血清C-反应蛋白水平比较,经t检验,差异有统计学意义(P<0.05),种植体周围炎组患者尿脱氧吡啶啉含量和血清C-反应蛋白水平均高于健康种植体组。见表5。
2.6 种植体周围炎组和健康种植体组患者血清C-反应蛋白水平与尿脱氧吡啶啉含量的相关性
种植体周围炎组和健康种植体组患者血清C-反应蛋白水平与尿脱氧吡啶啉含量呈正相关(r= 0.341和0.352,P=0.000)。
表3 种植体周围炎组与对照组的尿脱氧吡啶啉含量和血清C-反应蛋白水平比较 (n=60,mg/L,±s)

表3 种植体周围炎组与对照组的尿脱氧吡啶啉含量和血清C-反应蛋白水平比较 (n=60,mg/L,±s)
注:1)与术前比较,P<0.05;2)与术后比较,P<0.05
组别 尿脱氧吡啶啉 血清C-反应蛋白种植体周围炎组术前6.61±1.211.11±0.26术后1个月7.89±1.451) 18.32±6.571)对照组F值P值6.62±1.122)1.01±0.192)16.324 536.251 0.000 0.000
表4 健康种植体组与对照组的尿脱氧吡啶啉含量和血清C-反应蛋白水平比较 (n=60,mg/L,±s)
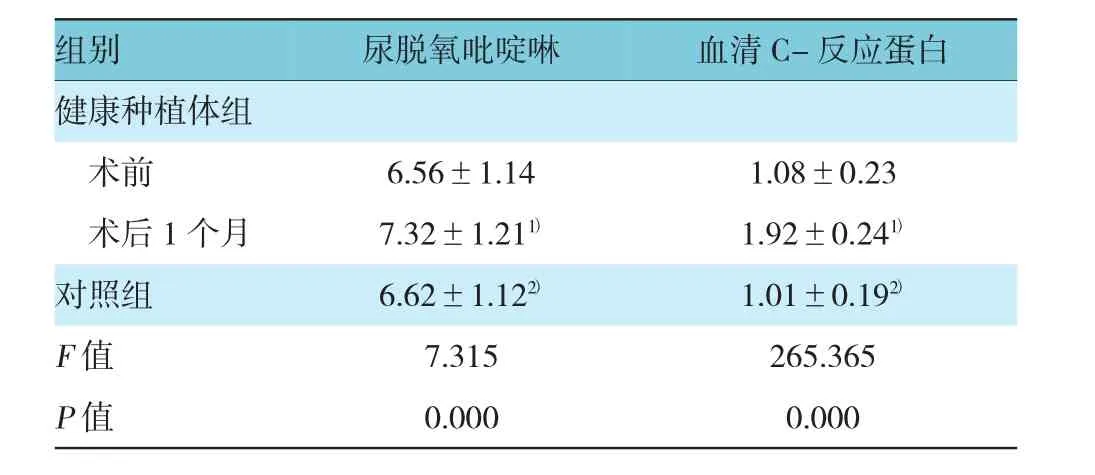
表4 健康种植体组与对照组的尿脱氧吡啶啉含量和血清C-反应蛋白水平比较 (n=60,mg/L,±s)
注:1)与术前比较,P<0.05;2)与术后比较,P<0.05
组别 尿脱氧吡啶啉 血清C-反应蛋白健康种植体组术前6.56±1.141.08±0.23术后1个月 7.32±1.211) 1.92±0.241)对照组1.01±0.192)F值 7.315 265.365 P值 0.000 0.000 6.62±1.122)
表5 种植体周围炎组和健康种植体组术后尿脱氧吡啶啉含量和血清C-反应蛋白水平比较 (n=60,mg/L,±s)
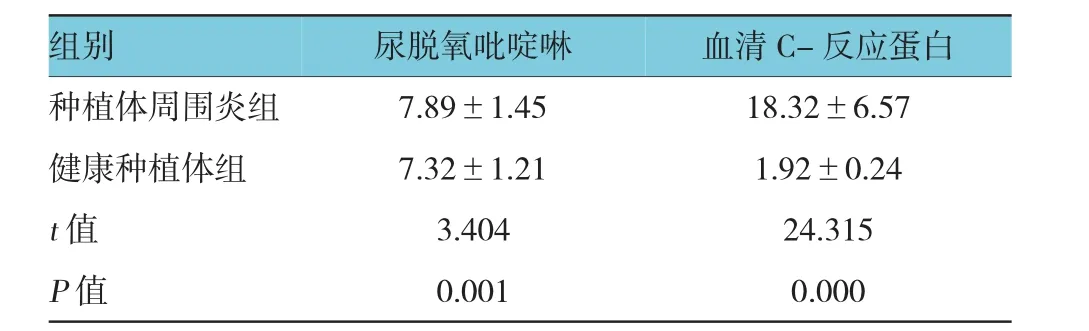
表5 种植体周围炎组和健康种植体组术后尿脱氧吡啶啉含量和血清C-反应蛋白水平比较 (n=60,mg/L,±s)
组别 血清C-反应蛋白种植体周围炎组 7.89±1.45 18.32±6.57健康种植体组 7.32±1.21 1.92±0.24 t值 3.404 24.315 P值 0.001 0.000尿脱氧吡啶啉
3 讨论
随着口腔种植技术的普及,种植体周围炎等并发症的发生率明显升高,种植体周围炎的两大特点为骨吸收和炎症反应,种植体植入牙槽骨到种植体修复完成,牙槽骨均处于改建吸收过程,而牙槽骨的改建吸收无法通过肉眼和辅助检查观察到。C-反应蛋白是敏感的炎症反应指标,在严重骨吸收及急性骨损伤时C-反应蛋白也会升高[7-9],邱大鹏等[10]研究发现,慢性眼轴患者龈沟液中C-反应蛋白浓度与牙周破坏程度有关,牙周基础治疗后龈沟液中C-反应蛋白水平下降。在骨代谢过程中,破骨细胞降解骨组织中的Ⅰ型胶原纤维产生脱氧吡啶啉,脱氧吡啶啉是骨代谢性疾病、全身骨转化的重要检测指标[11-13]。本研究结果发现,健康种植体患者术前尿脱氧吡啶啉含量和血清C-反应蛋白水平与对照组比较,差异无统计学意义;术后1个月时,尿脱氧吡啶啉含量和血清C-反应蛋白水平高于对照组。可见种植体植入后,在牙槽骨吸收改建的高峰期,尿脱氧吡啶啉含量和血清C-反应蛋白水平升高,考虑其原因为脱氧吡啶啉含量和C-反应蛋白水平和牙槽骨的吸收重建关系密切。
种植体周围炎是种植失败的主要原因,是由细菌感染所导致,临床上种植体周围组织的健康状况主要通过肉眼观察和影像学检查判断,肉眼观察主观性比较强,缺乏客观数据,影像学检查对种植体周围炎的判断具有滞后性。C-反应蛋白为炎症性疾病和存在感染时的急性时相反应蛋白,是主要的炎症标志物,在机体发生炎症反应是,C-反应蛋白迅速升高。大量研究发现,血清C-反应蛋白和牙周炎关系密切[14-15]。种植体周围炎时尿脱氧吡啶啉含量和血清C-反应蛋白水平升高,种植体周围炎的发生可能与脱氧吡啶啉含量及血清C-反应蛋白水平关系密切。种植体周围炎时C-反应蛋白升高的可能原因为:①种植体周围炎是一种感染性疾病,急性期引起机体释放大量炎症细胞因子,炎症细胞因子引起C-反应蛋白的合成增加,C-反应蛋白释放入血,引起血清C-反应蛋白水平的升高;②种植体周围炎伴有周围软组织的急性损伤及牙槽骨的吸收,机体处于应激状态,机体的应激反应需要C-反应蛋白的参与,使肝细胞合成C-反应蛋白增多,进入血液循环导致血清C-反应蛋白水平的升高。种植体周围炎时尿脱氧吡啶啉的含量增加考虑可能原因为:种植体周围炎时,牙槽骨的吸收比较活跃,破骨细胞降解骨组织中的Ⅰ型胶原纤维产生脱氧吡啶啉,脱氧吡啶啉的增加通过代谢进入尿液,使尿液中脱氧吡啶啉的含量增加。由此可见,种植体周围炎时尿脱氧吡啶啉含量和血清C-反应蛋白高于健康种植体患者,尿脱氧吡啶啉含量和血清C-反应蛋白可以反应种植体周围炎的炎症状况,种植体修复患者若术后尿脱氧吡啶啉含量和血清C-反应蛋白水平升高明显应警惕种植体周围炎的发生。
综上所述,人工种植牙修复术后健康种植体和种植体周围炎患者的尿脱氧吡啶啉含量和血清C-反应蛋白水平升高可能与牙槽骨的吸收重建有关。
[1]SATO R,ONDA K,KATO H,et al.An evaluation of the effect of age and the peri-parturient period on bone metabolism in dairy cows as measured by serum bone-specific alkaline phosphatase activity and urinary deoxypyridinoline concentration[J]. Vet J,2013,197(2):358-362.
[2]SHI J,WANG Z,LI H,et al.Diagnostic performance of the urinary deoxypyridinoline in spinal tuberculosis[J].Orthopedics, 2012,35(6):e922-e926.
[3]张玲莉,陈炳霖,邹军.运动影响骨转换:促进或抑制骨细胞/破骨细胞的发育和活性[J].中国组织工程研究,2014,18(42):6838-6843.
[4]LING M R,CHAPPLE I L,MATTHEWS J B.Neutrophil superoxide release and plasma C-reactive protein levels pre-and postperiodontal therapy[J].J Clin Periodontol,2016,43(8):652-658.
[5]REDMAN R S,KERR G S,PAYNE J B,et al.Salivary and serum procalcitonin and C-reactive protein as biomarkers of periodontitis in united states veterans with osteoarthritis or rheumatoid arthritis[J].Biotech Histochem,2016,91(2):77-85.
[6]ARDILA C M,GUZM魣N I C.Comparison of serum amyloid A protein and C-reactive protein levels as inflammatory markers inperiodontitis[J].J Periodontal Implant Sci,2015,45(1):14-22.
[7]SAKELLARIOU G T,ANASTASILAKIS A D,BISBINAS I,et al. Circulating periostin levels in patients with AS:association with clinicaland radiographic variables,inflammatory markersand molecules involved in bone formation[J].Rheumatology(Oxford), 2015,54(5):908-914.
[8]ZUZA E P,BARROSO E M,FABRICIO M,et al.Lipid profile and high-sensitivity C-reactive protein levels in obese and non-obese subjects undergoing non-surgical periodontal therapy[J]. J Oral Sci,2016,58(3):423-430.
[9]BASER U,OZTEKIN G,ADEMOGLU E,et al.Is the severity of periodontitis related to gingival crevicular fluid and serum high-sensitivity C-reactive protein concentrations[J].Clin Lab, 2014,60(10):1653-1658.
[10]邱大鹏,张倩,陈斌,等.牙周非手术治疗对重度慢性牙周炎患者龈沟液中C反应蛋白的影响[J].口腔医学,2016,36(10):876-879.
[11]EL-DORRY G,ASHRY H,IBRAHIM T,et al.Bone density, osteocalcin and deoxypyridinoline for early detection of osteoporosis in obese children[J].Open Access Maced J Med Sci, 2015,3(3):413-419.
[12]DEMIR M,ULAS T,TUTOGLU A,et al.Evaluation of oxidative stress parameters and urinary deoxypyridinoline levels in geriatric patients with osteoporosis[J].J Phys Ther Sci,2014,26(9): 1405-1409.
[13]RUITER R,OEI L,VISSER L E,et al.The effect of thiazide and loop diuretics on urinary levels of free deoxypyridinoline: an osteoclasticbone-resorption marker[J].J Clin Pharm Ther, 2013,38(3):225-229.
[14]GOYAL L,BEY A,GUPTA N D,et al.Comparative evaluation of serum C-reactive protein levels in chronic and aggressive periodontitispatients and association with periodontaldisease severity[J].Contemp Clin Dent,2014,5(4):484-488.
[15]田亚光,邱乐宏,陈小滨,等.牙周基础治疗对患牙周炎孕妇C反应蛋白的影响[J].大连医科大学学报,2015,37(2):142-144.
(童颖丹 编辑)
Changes of deoxypyridinoline and C-reactive protein before and after artificial dental implant restoration
Zhong-peng Li1,Hui-ping Wei2,Hua Chen3,Qi-sheng Wei3
(1.Integrated Outpatient Department,Stomatological Hospital Affiliated to Guangxi Medical University,Nanning,Guangxi 530021,China;2.Department of Stomatology,People's Hospital of Guangxi Zhuang Autonomous Region,Nanning,Guangxi 530021,China; 3.Stomatological Hospital of Guilin,Guilin,Guangxi 541001,China)
ObjectiveTo investigate the changes of urinary deoxypyridinoline and serum C-reactive protein before and after artificial dental implant restoration.MethodsIn this study,60 cases of peri-implantitis in Guangxi area from July 2011 to June 2016 were collected as peri-implantitis group,60 cases of healthy implants were collected as healthy implant group,and 60 healthy people were collected as control group.The urinary deoxypyridinoline content and serum C-reactive protein level were determined.ResultsThere was no significant difference in urinary deoxypyridinoline content or serum C-reactive protein level among the three groups before operation (P>0.05).The levels of urinary deoxypyridinoline and serum C-reactive protein after operation in the peri-implantitis group were higher than those before operation and in the control group (P< 0.05).The levels of urinary deoxypyridinoline and serum C-reactive protein at 1 month after implantation in the healthy implant group were higher than those before operation and in the control group (P<0.05).The levels of urinary deoxypyridinoline and serum C-reactive protein in the peri-implantitis group were higher than those in the healthy implant group at 1 month after implantation (P<0.05).There was a positive correlation between serum C-reactive protein level and urinary deoxypyridinoline content in the peri-implantitisgroup and the healthy implant group (P<0.05).ConclusionsThe levels of urinary deoxypyridinoline and serum C-reactive protein are significantly increased in the patients with peri-implantitis after artificial dental implant restoration.The levels of urinary deoxypyridinoline and serum C-reactive protein of the patients with healthy implants after artificial dental implant restoration are also increased.
oral implant repair;peri-implantitis;urinary deoxypyridinoline;C-reactive protein.
R783.6
A
10.3969/j.issn.1005-8982.2017.09.024
1005-8982(2017)09-0113-04
2017-02-13
猜你喜欢
北京大学学报(医学版)(2022年1期)2022-04-14
口腔医学(2021年10期)2021-12-02
中老年保健(2021年3期)2021-08-22
天津医科大学学报(2021年2期)2021-03-29
中国药学药品知识仓库(2021年18期)2021-02-28
昆明医科大学学报(2021年1期)2021-02-07
昆明医科大学学报(2021年1期)2021-02-07
现代临床医学(2021年1期)2021-01-26
CHINESE JOURNAL OF AERONAUTICS(2016年3期)2016-11-23
医学研究杂志(2015年7期)2015-06-22