
The effects of total ankle replacement on ankle joint mechanics during walking
2017-09-21 11:54HenryWangScottBrownb
Henry Wang*,Scott R.Brownb
aBiomechanics Laboratory,School of Kinesiology,Ball State University,Muncie,IN 47306,USA
bSports Performance Research Institute New Zealand(SPRINZ),Auckland University of Technology,Auckland 1020,New Zealand
The effects of total ankle replacement on ankle joint mechanics during walking
Henry Wanga,*,Scott R.Browna,b
aBiomechanics Laboratory,School of Kinesiology,Ball State University,Muncie,IN 47306,USA
bSports Performance Research Institute New Zealand(SPRINZ),Auckland University of Technology,Auckland 1020,New Zealand
Background:End-stage ankle arthritis impairs joint function and patients’mobility.Total ankle replacement is a surgical procedure to treat severe ankle arthritis.Salto Talaris Anatomic AnkleTM(STAA)was designed to mimic the normal ankle anatomy and flexion/extension of the ankle movement.The purpose of this study was to examine the effect of an STAA ankle replacement on ankle joint function and mechanics during gait. Methods:Five patients with end-stage unilateral ankle arthritis were recruited.Patients performed level walking in a laboratory setting on 2 occasions,prior to and 3 months after the STAA ankle surgeries.American Orthopedic Foot and Ankle Society(AOFAS)hindfoot score was obtained.A 12-camera motion capture system was used to perform walking analysis.Gait temporo-spatial parameters and ankle joint mechanics were evaluated.Paired Student’s t tests and non-parametric Wilcoxon matched tests were performed to examine the differences in biomechanical variables between the pre-and post-surgery walking conditions.
Results:Compared to the pre-surgical condition,at 3 months of post-STAA surgery,patients experienced greater improvement inAOFAS hindfoot score(p=0.0001);the STAA ankle demonstrated a 31%increase in ankle joint excursion(p=0.045),a 22%increase in ankle plantar flexor moment(p=0.075),a 60%increase in ankle power absorption(p=0.023),and a 68%increase in ankle power production(p=0.039).Patients also demonstrated a 26%increase in walking speed(p=0.005),a 20%increase in stride length(p=0.013),a 15%decrease in double support time (p=0.043),and a 5%decrease in total stance time(p=0.055).
Conclusion:Three months after surgeries,the STAA patients experienced improvements in ankle function and gait parameters.The STAA ankle demonstrated improved ankle mechanics during daily activities such as walking.
©2017 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Ankle mechanics;AOFAS score;Arthritis;Gait analysis;Total ankle replacement;Walking
1.Introduction
Ankle joint arthritis is a progressive cartilage degenerative disease,which is signi fied by pain,limited range of motion,and stiffness.Over 70%of ankle joint arthritis is a result of joint traumas such as ankle fractures and ligament ruptures.1Rheumatoid arthritis and osteoarthritis account for the rest of the percentages of ankle joint arthritis.1Currently,over 1%of the adult population suffers ankle joint arthritis worldwide.2
End-stage ankle arthritis impairs ankle joint function and results in physical disabilities.Due to the effectiveness of reducing joint pain and improving patients’mobility,anklearthrodesis(ankle joint fusion)has been an important treatment method for patients with end-stage ankle arthritis.3It was reported that ankle arthrodesis results in satisfactory outcomes and acceptable gait function.4–7However,there were limitations associated with ankle arthrodesis.Firstly,the tibio–talar joint is fused and loses its motion,which causes compensatory motion and increased mechanical stress at other associated parts of the foot and leg.In the long term,the risk of developing subtalar and midtarsal degenerative joint disease is thus increased.8,9Secondly,patients with arthrodesis develop compensatory walking patterns and demonstrate asymmetrical gait.5In the past 40 years,total ankle replacement(TAR)has become an alternative of arthrodesis for the treatment of severe ankle arthritis.TAR can eliminate ankle joint pain and return ankle joint to function.8,10Although there is still a debate whether one procedure is better than the other,4,7,10,11TAR does havesome advantages over ankle arthrodesis.Compared to a fused ankle joint,a TAR could restore normal ankle range of motion resulting in a less compromised gait.12Also,adverse effects on the other joints of the same limb are less likely to occur.
Early TAR designs were two-component designs that included a tibial component and a talar component.Both components were constrained to allow 1°of freedom of motion. The outcomes of constrained two-component TARs were not satisfactory due to component loosening and failures.13,14In the 1990s,the development of an unconstrained,meniscal bearing type of TAR had led to improved clinical outcomes.15–17The mobile-bearing three-component TAR design is characterized with metal tibial and talar components articulating with an unattached polyethylene meniscus.Mobile bearing TARs represented by the Salto mobile-bearing TAR(Tornier Inc., Montbonnot Saint Martin,France)have achieved a 93%survivorship at 6.4 years follow-up and an 85%survivorship at 8.9 years follow-up.18,19In recent years,based on the success of the Salto mobile-bearingTAR,the SaltoTalarisAnatomicAnkleTM(STAA)(Tornier Inc.)was introduced to customers in the US. The STAA is characterized with unconstrained tibial and talar components and a polyethylene insert secured to the metal tibial component.This two-component STAA is a new generation TAR that mimics the anatomy and flexion/extension movement of the normal ankle joint(http://www.tornier-us.com/ lower/ankle/ankrec004/).Speci fically,the talar implant mimics the anatomy of the talar dome and the flexion/extension axis is the axis of a cone to allow normal external rotation of the foot during dorsi flexion.
To date,there are no studies that report on the kinematic or kinetic changes that occur with the STAA system.It is not known how quickly a patient could gain ankle function and strength after receiving the STAA.It is not clear whether the STAA could improve patients’ability to perform daily activities (e.g.,level walking).Therefore,the purpose of this study was to examine the ankle joint function and mechanics during level walking in patients with unilateral ankle arthritis on the following 2 occasions:pre-and 3 months post-surgery with the STAA.It was hypothesized that the TAR joint would demonstrate improved clinical and functional outcomes,gait parameters,and ankle joint mechanics when compared to the same limb before surgery during level walking.
2.Methods
Five patients(3 males and 2 females;67±6 years,91±17 kg, 173±7 cm,mean±SD)who developed unilateral ankle osteoarthritis due to severe ankle joint injuries(e.g.,ankle fractures and sprains)volunteered in the study.All patients were diagnosed with advanced,end-stageanklearthritis(Grades2–3basedonCanadian Orthopaedic Foot and Ankle Society classi fication20)before TAR surgeries.Standard surgical procedure for installing fixed bearing TARs was performed.Patients had gone through a standard rehabilitation protocol after the surgeries.Speci fically,for the first 6 weeks of postoperation,patients wore walker boots;from the 2nd to the 10th week,patients performed active range of motion exercise at the ankle and strength exercises of the core,hip,and knee joints;fromthe6thtothe10thweek,scarmassagewasconducted; stationary biking exercise was introduced;patients also practiced weight-bearing activities including standing,weight shifting,and short distance walking;from the 10th to the 16th week,patients continued their gait training and strength training of core,hip, knee,and ankle;patients also started unilateral stance exercises, bilateral heel raises,and balance exercises.This study was approved by Institutional Review Board at Ball State University. All subjects were informed of the study procedures and signed informed consent forms prior to participation in the study.
Patients’clinical and functional outcomes were assessed by an experienced physical therapist via theAmericanOrthopaedic Foot and Ankle Society(AOFAS)hindfoot score system.21During the assessment,ankle joint pain,function,hindfoot motion,and joint alignment were evaluated with a maximum score of 100.
Three-dimensional(3D)trajectories of re flective markers placed on the body were captured during testing trials using a 12-camera(MX 40)motion capture system(100 Hz)(VICON Inc.,Denver,CO,USA).Ground reaction forces were also collected(1000 Hz)during testing trials using 2 embedded AMTI force platforms(Model OR6-7-2000;Advanced Mechanical Technologies Inc.,Watertown,MA,USA).VICON Workstation(Version 5.2.4;VICON Inc.)was used to reconstruct and process the raw 3D trajectory data and ground reaction force data.
Subjects came to the Ball State University Biomechanics Laboratory on 2 separate occasions for the study:pre-and 3 months post-TAR surgery(all performed by the same surgeon) using the STAA in the affected ankle.During both visits, subjects followed identical testing protocols.Subject anthropometrics were gathered and then spherical retrore flective markers(14 mm)were fitted bilaterally on speci fic lower extremity anatomical landmarks following the Plug-in-Gait model protocol.Subjects then performed a general 5 min warm-up on a stationary bike before testing trials.Next,subjects were instructed to perform level walking gait trials at a self-selected pace within the gait analysis walkway(approximately 10 m in length).Walking movement was performed in a barefoot condition.Trials were deemed acceptable if the foot of interest landed completely on the force platform and the subject maintained a consistent gait pattern.A minimum of 5 trials were required to come from the affected ankle.
VICONWorkstation(Version5.2.4)wasusedtogenerategait temporo-spatialparameterssuchaswalkingspeed,stridelength, stancetime,anddoublesupport.Inaddition,anklejointmechanicsincludingmaximaldorsi flexion,maximalplantar flexion,and joint excursion(joint range of motion from peak dorsi flexion to peak plantar flexion during stance of gait),peak ankle joint moment,andpeakanklejointpowerwereanalyzedforbothpreand post-TAR surgeries.Standard inverse dynamic calculations were performed to obtain joint moments and powers.22Stance timeanddoublesupporttimewerenormalizedtoafullgaitcycle (identi fied as heel strike of the affected ankle to the next heel strike of the same ankle).Ankle joint moments and powers were normalized to body mass.
Statistical analysis was performed using SPSS software for Windows(Version 19.0;IBM Corp.,Armonk,NY,USA).Dependent variables includedAOFAS hindfoot scores,walking speed,stride length,stance time,double support time,peak dorsi flexion,peak plantar flexion,ankle excursion,peak ankle moment and power during stance.Shapiro–Wilk normality tests were used to verify whether data were normally distributed. Paired Student’s t tests and non-parametric Wilcoxon matched paired tests were used for data comparison between the pre-and post-surgery conditions in normally and non-normally distributed data,respectively.All signi ficant levels were set at 0.05.
3.Results
The AOFAS hindfoot score at 3 months of post-surgery (74±10)was signi ficantly greater than that of the pre-surgery condition(48±17)(p=0.0001).
The involved and contralateral ankle joint mechanics are presented in Table 1.Fig.1 shows the involved ankle joint’s angle,moment,and power during stance phase of walking. Three months after ankle surgery,subjects were able to signi ficantly improve the ankle joint mechanics during gait.Speci fically,compared to the pre-surgical condition,at 3-month mark post-TAR surgery,the TAR limb demonstrated a 31%increase in ankle joint excursion(p=0.045),a 60%increase in peak ankle power absorption(p=0.023),and a 68%increase in peak ankle power production(p=0.039).Although it was not statistically signi ficant(p=0.075),the peak ankle plantar flexor moment at 3 months of post-surgery was 22%greater than that of the pre-surgical condition with 4 out of 5 patients seeing improvements.
Gait temporo-spatial parameters of pre-and 3 months post-TAR surgeries are presented in Table 2.Three months after ankle surgery,subjects were able to signi ficantly improve temporo-spatial gait parameters from their pre-surgical conditions.Speci fically,when compared to the pre-surgery walking, during the post-surgery walking,subjects demonstrated a 26% increase in walking speed(p=0.005),a 20%increase in stride length(p=0.013),and a 15%decrease in double support time (p=0.043).In addition,there is a trend(p=0.055)showingthat the total stance time was reduced by 5%from the presurgical condition to the 3 months post-surgical condition.
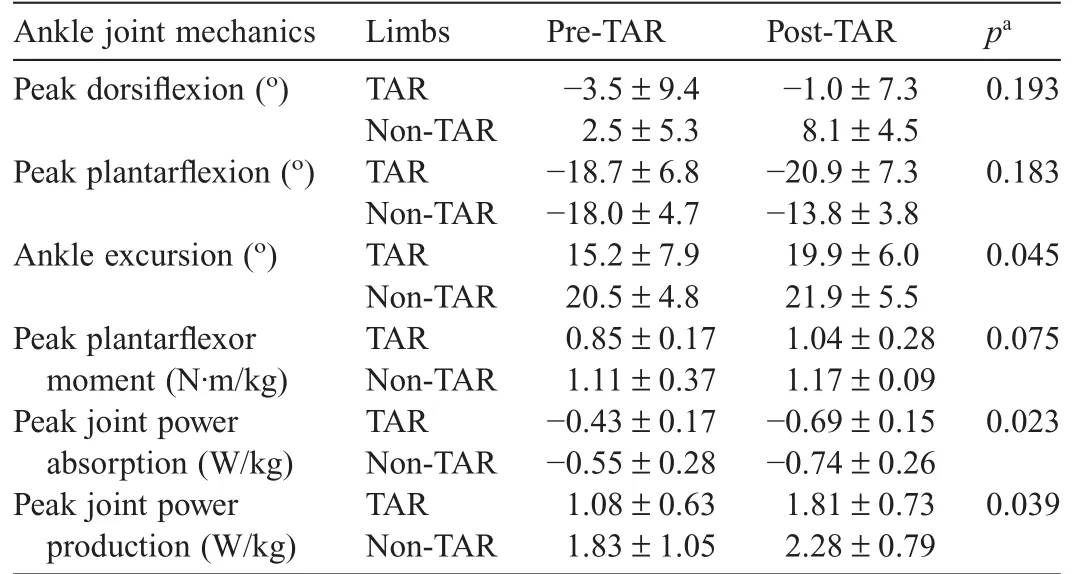
Table 1 The involved and contralateral ankle joint mechanics during pre-and 3-month post-surgery walking(mean±SD).
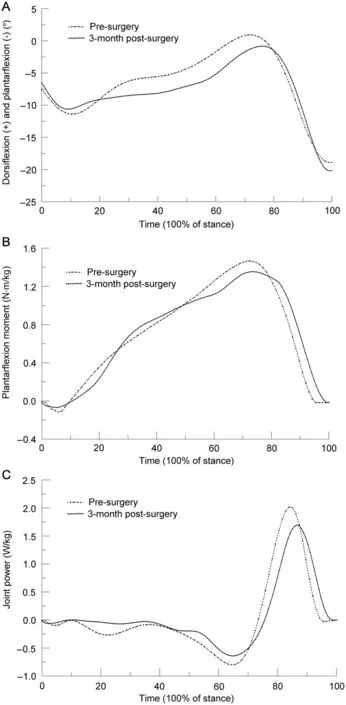
Fig.1.(A)Ankle joint angles in sagittal plane,(B)ankle joint plantar flexor moment,and(C)ankle joint power during stance of walking.Data were taken from a typical trial of a participant.
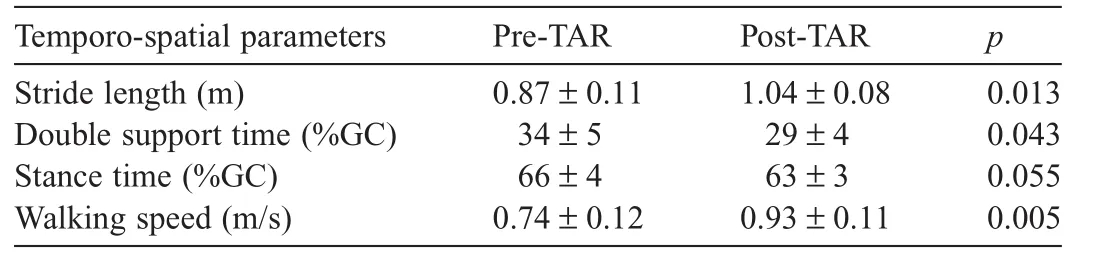
Table 2 The temporo-spatial parameters during pre-and 3-month post-surgery walking (mean±SD).
4.Discussion
A TAR procedure is used to treat end-stage ankle joint arthritis to eliminate joint pain and improve joint mechanics during daily activities.An STAA is designed to restore normal ankle joint anatomy and function.It is not clear whether an STAA could result in pronounced improvements of ankle joint mechanics in 3 months.The purpose of the study was to examine the effect of an STAA surgery on ankle joint mechanics during level walking at the 3-month mark post-surgery.We expected to observe positive changes in ankle clinical and functional scores,ankle joint mechanics and gait parameters after 3 months of surgery.Results from this laboratory testing confirmed our expectations.
The TAR patients had a signi ficant increase of AOFAS hindfoot score in 3 months after the TAR surgeries.This pronounced increase in AOFAS hindfoot score demonstrates that theTAR procedure could successfully alleviate ankle joint pain, improve ankle function,increase hindfoot motion,and restore joint alignment.Similar findings were reported by Barg et al.23and Haddad et al.4Barg et al.23followed 388 patients(mean age:63 years)with end-stage ankle arthritis.They found that after 4 years ofTAR surgeries,patients’AOFAS hindfoot score was improved from 39 to 76.Haddad et al.4performed a systematic review on surgical treatments for patients with endstage ankle arthritis from 1990 to 2005.They reported the AOFAS scores of 243 patients(mean age:58 years)with TAR and 136 patients(mean age:50 years)with ankle arthrodesis. Two years after ankle surgery,patients withTAR had anAOFAS hindfoot score of 78 and patients with ankle arthrodesis had a score of 76.In the current study,anAOFAS hindfoot score of 74 is comparable to findings from the above studies.4,23Moreover, as ankle joint strength was expected to continue to improve beyond the 3-month mark post-surgery,patients with the STAA could have the potential to further increase theAOFAS score in longer terms(e.g.,in 6 months and 1 year after surgeries).
We had hypothesized that the TAR limb would demonstrate improved ankle joint mechanics during level walking.This hypothesis was supported.Compared to their pre-surgical conditions,3 months after ankle surgery,patients were able to produce greater ankle joint excursion,peak joint power absorption,and peak joint power production during stance of a gait cycle.Ankle joint plays an important role in human walking. During the loading response of the stance phase,the ankle joint acts to absorb ground impact forces.24Speci fically,to prevent the foot from slapping on the ground and to lessen the impact loading,the dorsi flexor(tibialis anterior)controls the ankle joint’s plantar flexion motion through eccentric contractions.24When the foot is flat on the ground,the ankle joint moves into dorsi flexion while the plantar flexors contract eccentrically to control the forward advancement of the lower leg over the foot. During this single support phase,there is power absorption in the ankle and the plantar flexors store elastic energy through lengthening.In this study,prior to ankle surgery,patients exhibited a signi ficant reduction of peak joint power absorption during single support.The impaired ankle joint anatomy and function reduces the rate of energy absorption at plantar flexors. In just 3 months after joint replacements,patients were able to show an increase in peak ankle power absorption,which re flected an improvement in ankle joint function.Furthermore, the plantar flexors(soleus and gastrocnemius)are the leg muscles making signi ficant contributions to the forward progression of the body during walking.25Prior to ankle surgery, patients walked with a reduced ankle range of motion.The ankle joint pain and a reduced range of motion from arthritis had impaired the plantar flexors’ability to produce adequate net muscle moment and power to propel the body forward.Three months after ankle replacement,patients all demonstrated signi ficant improvements in ankle range of motion and joint power. In addition,4 out of 5 patients demonstrated an increase in peak plantar flexor moment.It is possible that the restored ankle joint anatomy and range of motion allow the plantar flexors to produce large ankle moment and power to move the body forward.Thus,it is evident that the STAA could effectively improve ankle joint mechanics during walking.Interestingly, Valderrabano et al.26conducted a study evaluating gait changes of patients with end-stage ankle OA preoperatively and in the first year after the TAR surgery with a HINTEGRATMTAR system(Newdeal SA,Lyon,France).While their patients’AOFAS score was found to improve from 34 preoperatively to 93 one year after surgery,they reported that patients experienced a worsened gait at 3-month follow-up.In particular,the peak ankle joint plantar flexor moment and peak ankle power were down 12%and 15%from the preoperative condition, respectively.This finding appears to be contradictive to our results,which indicate a trend of an increase in peak plantar flexor moment(a 22%increase)and a pronounced improvement in ankle power(a 68%increase).It is unclear what factors contribute to the differences in findings between our study and Valderrabano’s study.26One possible reason may be related to differences in TAR designs and procedures.The HINTEGRATMTAR system tested in Valderrabano’s study26is a three-component mobile bearing TAR.The STAA system used in this study is a two-component fixed bearing TAR.Surgical techniques used to install a mobile bearing TAR may be more complicated than installing a fixed bearing TAR.Additional bone and soft tissue damages may be introduced during the HINTEGRATMTAR procedure and perhaps lead to an increase in recovery time exceeding the 3-month mark postsurgery.Unfortunately,in the study,patients’AOFAS score was not measured at the 3-month mark post-surgery.It is unclear whether the worsened gait mechanics corresponded to a poor AOFAS score at 3-month post-operation.Future studies are needed to determine the in fluences of different TAR designs and surgical procedures on ankle joint mechanics as well as their long-term effects on ankle function.
We had also hypothesized that there would be improved temporo-spatial gait parameters after the TAR surgeries.Our hypothesis was supported.We found that there were longer stride length,shorter stance time and double support time,and faster walking speed associated with the post-surgery walking. These improved temporo-spatial parameters were in factconsistent with the improved ankle joint mechanics after the surgeries.During the pre-surgery walk,it was found that patients experienced ankle pain and a limited range of motion. They lengthened the double support time to ensure a smooth execution of body weight transfers from one limb to another. The entire stance time was also lengthened to allow the plantar flexors to generate enough impulse on the ground to move the body forward.The stride length was reduced due to the inability of the plantar flexors to produce a large joint moment.Subsequently,walkingspeedwassigni ficantly reduced.However,with the assistance of an STAA system, compared to the pre-surgical condition,theTAR limb improved ankle function in as short as 3 months and was able to produce a 22%more ankle plantar flexor moment and 68%more ankle joint power at push-off.The pronounced increase of ankle joint power contributed to a 20%longer stride and 26%faster walking speed.In addition,as the ankle joint function improved,the surgical limb did not need to spend more time on the ground to generate necessary impulse to gain walking speed.Decreased stance time and double support time in conjunction with an increased stride length had led to a pronounced increase of walking speed.Thus,it is evident that the STAA can improve an arthritic joint’s function signi fied by improvements in temporo-spatial parameters.In this study,we did not include a healthy control group to examine the differences between TAR patients and healthy subjects.In a study conducted by Valderrabano et al.,26a healthy control group was tested.The average walking speed and stride length of the healthy controls were 1.29 m/s and 1.35 m,respectively.Apparently,our patients walked at a slower speed(0.93 m/s)with a shorter stride length (1.04 m)than the control group at 3-month follow-up.In addition,the patient group in Valderrabano’s study26had a walking speed of 1.02 m/s and a stride length of 1.23 m,which were also greater than those of our patients.The differences in gait parameters such as walking speed and stride length between our patients and the cohorts in Valderrabano’s study may be due to a difference in age.Our patients were older than those recruited in Valderrabano’s study(67 years vs.53 years)and might possess weaker lower extremity strength.Nonetheless,it is expected that as lower extremity function and strength continue to improve,patients in this study could further improve their temporo-spatial gait parameters.
Limitations of the study must be addressed.The sample size used in the study was small;we were only able to recruit 5TAR patients to test their gait in pre-and 3-month post-surgical conditions.In addition,we did not perform mid-and long-term evaluations on our patients’gait.It is necessary to conduct studies to examine the long-term effect of the STAA on walking mechanics.
5.Conclusion
The STAA appears to help patients improve ankle joint function.Three months after the STAA surgery,patients were able to increase ankle joint range of motion and peak joint power,and subsequently increase walking speed.Future research should examine the longevity of the STAA in order to eliminate a further revision and to firmly establish its long-term bene fits and functionality.
Acknowledgment
We thank Steven A.Herbst,MD,from Central Indiana Orthopedics for his contribution to the organization and support of the study,and Jeff Frame from Ball State University for his assistance with the data collection.No funding was received for this study.
Authors’contributions
HW participated in study design,subject recruitment,data collection,data processing,data analysis,and drafted the manuscript;SRB participated in data processing and data analysis, and helped draft the manuscript.Both authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
1.Saltzman CL,Salamon ML,Blanchard GM,Huff T,Hayes A,Buckwalter JA,et al.Epidemiology of ankle arthritis:report of a consecutive series of 639 patients from a tertiary orthopaedic center.Iowa Orthop J 2005;25: 44–6.
2.Glazbrook M,Daniels T,Younger A,Foote CJ,Penner M,Wing K,et al. Comparison of health-related quality of life between patients with end-stage ankle and hip arthrosis.J Bone Joint SurgAm 2008;90:499–505.
3.Nihal A,Gellman RE,Embil JM,Trepman E.Ankle arthrodesis.J Foot Ankle Surg 2008;14:1–10.
4.Haddad SL,Coetzee JC,Estok R,Fahrbach K,Banel D,Nalysnyk L. Intermediate and long-term outcomes of total ankle arthroplasty and ankle arthrodesis,a systematic review of the literature.J Bone Joint Surg Am 2007;89:1899–905.
5.Piriou P,Culpan P,Mullins M,Cardon JN,Pozzi D,Judet T.Ankle replacement versus arthrodesis:a comparative gait analysis study.Foot Ankle Int 2008;29:3–9.
6.Saltzman CL,Mann RA,Ahrens JE,Amendola A,Anderson RB,Berlet GC,et al.Prospective controlled trial of STAR total ankle replacement versus ankle fusion:initial results.Foot Ankle Int 2009;30:579–96.
7.Espinosa N,Klammer G.Treatment of ankle osteoarthritis:arthrodesis versus total ankle replacement.Eur JTrauma Emerg Surg 2010;36:525–35.
8.Saltzman CL,McIff TE,Buckwalter JA,Brown TD.Total ankle replacement revisited.J Orthop Sports Phys Ther 2000;30:56–67.
9.Gould JS.Total ankle arthroplasty.Am J Orthop 2004;33:169–70.
10.Hahn ME,Wright ES,Segal AD,Orendurff MS,Ledoux WR,Sangeorzan BJ.Comparative gait analysis of ankle arthrodesis and arthroplasty:initial findings of a prospective study.Foot Ankle Int 2012;33:282–9.
11.Daniels TR,Younger A,Penner M,Wing K,Dryden PJ,Wong H,et al. Intermediate-term results of total ankle replacement and ankle arthrodesis, a COFAS multicenter study.J Bone Joint Surg Am 2014;96:135–42.
12.Doets H,Brand R,Nelissen R.Total ankle arthroplasty in in flammatory joint disease with the use of two mobile-bearing designs.J Bone Joint Surg Am 2006;88:1272–84.
13.Saltzman CL.Why ankle replacement?Clin Orthop Relat Res 2004;424:2.
14.Stengel D,Bauwens K,Ekkernkamp A,Cramer J.Ef ficacy of total ankle replacement with meniscal-bearing devices:a systematic review and meta-analysis.Arch Orthop Trauma Surg 2005;125:109–19.
15.Cracchiolo A,DeOrio J.Design features of current total ankle replacements:implants and instrumentation.JAmAcad Orthop Surg 2008; 16:530–40.
16.Buechel F,Poppas M.Survivorship and clinical evaluation of cementless, meniscal-bearing total ankle replacements.Semin Arthroplasty 1992; 3:43–50.
17.HintermannB,ValderrabanoV,DereymaekerG,DickW.The HINTEGRA ankle:rationale and short-term results of 122 consecutive ankles.Clin Orthop Relat Res 2004;424:57–68.
18.Bonnin M,Colombier J,Buscayret F,Graveleau N,Piriou P.Midterm results of the Salto Total Ankle Prosthesis.Clin Orthop Relat Res 2004; 424:6–18.
19.Bonnin M,Gaudot F,Laurent JR,Ellis S,Colombier JA,Judet T.The Salto total ankle arthroplasty.Survivorship and analysis of failures at 7 to 11 years.Clin Orthop Relat Res 2011;469:225–36.
20.Krause FG,Di Silvestro M,Penner MJ,Wing KJ,Glazebrook MA,Daniels TR,et al.Inter-and intra-observer reliability of the COFAS end-stage ankle arthritis classi fication system.Foot Ankle Int 2010;31:103–8.
21.Kitaoka HB,Alexander IJ,Adelaar RS,Nunley JA,Myerson MS.Clinical rating systems for the ankle-hindfoot,midfoot,hallux,and lesser toes.Foot Ankle Int 1994;15:349–53.
22.Winter D.Biomechanics and motor control of human movement.4th ed. Hoboken,NJ:John Wiley&Sons;2009.p.176–99.
23.Barg A,Knupp M,Hintermann B.Outcomes after total ankle replacement. Suomen Ortopedia ja Traumatologia 2013;36:46–53.
24.Rose J,Gamble J.Human walking.3rd ed.Philadelphia,PA:Lippincott Williams&Wilkins;2006.p.103–18.
25.Neptune RR,Kautz SA,Zajac FE.Contributions of the individual ankle plantar flexors to support,forward progression and swing initiation during walking.J Biomech 2001;34:1387–9.
26.Valderrabano V,Nigg BM,Tscharner V,Stefanyshyn DJ,Goepfert B, Hintermann B.Gait analysis in ankle osteoarthritis and total ankle replacement.Clin Biomech(Bristol,Avon)2007;22:894–904.
17 July 2014;revised 15 December 2014;accepted 21 September 2015
Available online 11 January 2016
Peer review under responsibility of Shanghai University of Sport.
*Corresponding author.
E-mail address:hwang2@bsu.edu(H.Wang)
http://dx.doi.org/10.1016/j.jshs.2016.01.012
2095-2546/©2017 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
 Journal of Sport and Health Science2017年3期
Journal of Sport and Health Science2017年3期
- Journal of Sport and Health Science的其它文章
- Time for a paradigm shift in the classi fication of muscle injuries
- Rehabilitation and return to sport after hamstring strain injury
- Risk factors for hamstring injuries in Australian male professional cricket players
- Relationships among hamstring muscle optimal length and hamstring flexibility and strength
- The effect of hamstring flexibility on peak hamstring muscle strain in sprinting
- Motivation dimensions for running a marathon:A new model emerging from the Motivation of Marathon Scale(MOMS)