
Preparatory training attenuates drastic response of the insulin-like growth factor binding protein 1 at the point of maximal oxygen consumption in handball players
2017-09-21 11:54OlgiNeiMilouneriGornMiljuZornVlevitVlimirJkovljeviMrijGlietiVesnVu
Olgi Nei´*,Miloš Šuneri´Gorn MiljušZorn Vlevit,Vlimir Jkovljevi´, Mrij Glieti´,Vesn Vuˇi´
aInstitute for the Application of Nuclear Energy,University of Belgrade,Belgrade 11080,Serbia
bFaculty of Sport and Physical Education,University of Belgrade,Belgrade 11000,Serbia
cDepartment of Physiology,Faculty of Medical Sciences,University of Kragujevac,Kragujevac 34000,Serbia
dCentre of Research Excellence in Nutrition and Metabolism,Institute for Medical Research,University of Belgrade,Belgrade 11000,Serbia
Preparatory training attenuates drastic response of the insulin-like growth factor binding protein 1 at the point of maximal oxygen consumption in handball players
Olgica Nedic´a,*,Miloš Šunderic´a,Goran Miljuša,Zoran Valdevitb,Vladimir Jakovljevic´c, Marija Glibetic´d,Vesna Vucˇic´d
aInstitute for the Application of Nuclear Energy,University of Belgrade,Belgrade 11080,Serbia
bFaculty of Sport and Physical Education,University of Belgrade,Belgrade 11000,Serbia
cDepartment of Physiology,Faculty of Medical Sciences,University of Kragujevac,Kragujevac 34000,Serbia
dCentre of Research Excellence in Nutrition and Metabolism,Institute for Medical Research,University of Belgrade,Belgrade 11000,Serbia
Background:Intensive exercise changes physiological need for glucose and several biochemical pathways responsible for its metabolism response. Among them are those which involve insulin,insulin-like growth factor(IGF-1),and IGF-binding proteins(IGFBPs).Different types and degrees of exercise,as well as an athlete’s fitness,may induce a range of responses regarding concentrations and time needed for the alteration.The idea of the work was to find out whether and how insulin/IGF axis responds to additional physical activity in the already trained subjects and if so,is the adaptation potentially bene ficial from the aspect of metabolic control.
Methods:The effect of 4-week intensive training on campus(preparatory training)on the levels of insulin,IGF-1,and IGFBPs during maximal progressive exercise test(MPET)on a treadmill was compared to the results obtained during MPET conducted after a regular training season of a female elite handball team(n=17,age:17±1 years,height:171±8 cm,weight:65±8 kg,body mass index:22±1 kg/m2at the beginning of the study;there were no signi ficant changes at the end).Serum samples were obtained from players immediately before the test(basal),at the end of the test after reaching the point of maximal oxygen consumption(VO2max),and after recovery.
Results:The concentration of insulin decreased at VO2max,but remained higher in players after preparatory training(12.2±2.5 mU/L vs. 8.9±4.4 mU/L,p=0.049).The level of IGFBP-1 decreased in players at VO2maxin either case of training,but it remained much higher in tests performed after the preparatory regime than before(p=0.029).Concentrations of IGF-1,IGFBP-2,-3,and-4 did not change signi ficantly.
Conclusion:The inverse relation between insulin and IGFBP-1 was lost during MPET,as these 2 molecules changed in the same direction.The results obtained suggest less severe stress-induced depression of insulin and IGFBP-1 after preparatory training.But another metabolic mechanism cannot be excluded,and that is potentially impaired insulin sensitivity resulting in higher level of IGFBP-1.
©2017 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Female;IGF-binding proteins(IGFBPs);Insulin;Insulin-like growth factor I(IGF-1);Progressive exercise test;VO2max
1.Introduction
Active training induces alterations of hormones and cytokines involved in the regulation of glucose concentration. In general,long-term training leads to reduced insulin concentration1and increased secretion of growth hormone(GH).2Results on the concentration of insulin-like growth factor 1(IGF-1),a mediator of GH activity,2and IGF-binding proteins(IGFBPs)are,however,contradictory. These molecules are involved in the regulation of glucose concentration,its utilization,and muscle growth and tissue repair.3
The close relationship between insulin and GH has been reviewed previously.4The physiological role of insulin is seen in lowering the concentration of glucose in blood,which is performed by 2 principal mechanisms—inhibition of glucoseproduction in the liver and stimulation of intracellular transport of glucose via speci fic membrane transporters.4Glucose transport is mainly driven by the concentration gradient,but insulin is responsible for controlling translocation of transporters on the cell surface.4Intracellular glucose is metabolized and the metabolites further enter the Krebs citric acid cycle,enabling energy release.5During exercise,this mechanism,together with the one stimulating glycogen breakdown to insure additional glucose,is activated.After exercise,with reduced need for energy release,insulin stimulates processes favoring conversion of glucose into“energy storage molecules”such as glycogen and fat.Insulin is responsible for the intracellular transport of amino acids as well,essential for protein synthesis and muscle recovery.Contrary to insulin,glucagon,epinephrine, cortisol,and GH are known as glucose-raising hormones.6IGF moleculescanbeseen as speci fically positioned in this network, as they are mediators of the anabolic function of GH and yet, they exert insulin-like activity.4
Increased concentration of IGF-1 was measured by several researchers after resistance training,alternating resistance exercise and running,long-term training in competitive swimmers, endurance exercise and in women involved in army physical training.7–14Decreased concentration of IGF-1 was reported in handballplayersandinhealthywomenafterstrength training.15,16Finally,Eliakim and colleagues17found no effect of volleyballpracticeinwomenonIGF-1;Meckeland co-workers18reported no effect of treadmill running on IGF-1 in handball players,and Nindl and his group19denied an effect of exercise on total,free,and bioactive IGF-1 in women.19
Similar inconsistency may be seen in the published results onIGFBPs.Intensivephysicalactivitywasfoundto increase,9,10,18decrease,8ornottoaffectIGFBP-3 concentration.7,16,17,19The concentration of IGFBP-1 was detectedtoincrease,20decrease,11,18orremain unchanged.8,10,16,19Less data are available on other IGFBPs,but they are opposing as well.IGFBP-2 was measured to increase,9decrease,11or stay unaltered due to exercise,19while IGFBP-4 and IGFBP-6 were reported to increase in army women.11Such enormous variation in the results on the IGF/IGFBP axis in athletesindicatesexercise-speci ficadaptation.Therefore, results obtained for 1 type of athlete cannot be extrapolated to others.
Handball is a globally popular team sport played by more than 30 million athletes all over the world.21It is a strenuous, intermittent physical activity that requires both aerobic and anaerobic power and endurance.22In spite of these facts,hormonal changes in handball players have been poorly studied, especially in female players.Thus,the aim of this study was to investigate changes in the insulin/IGF/IGFBP axis during maximal progressive exercise test(MPET)on treadmill performed by female elite handball team players after intensive training on campus(preparatory training)and to compare them with the response recorded after regular training.In accordance, it seemed relevant to find out whether and how insulin/IGF axis responds to additional physical activity in the already trained subjects and,if so,is the adaptation potentially bene ficial from the aspect of metabolic control.The first test was carried out immediately after the competition season,at the beginning of preparatory training and the second one after preparatory training,which lasted 4 weeks.We determined additional in fluence of preparatory training on the insulin/IGF/IGFBP axis,especially at the point of maximal oxygen consumption(VO2max), which is assumed to be the best single measure of aerobic fitness.23
2.Materials and methods
2.1.Participants
The study included 17 young female handball players,aged 16–18.The players were members of the Serbian national team, playing at national and international competitions.All of them were healthy,non-smokers and reported regular menstrual cycles(26–32 days).None of them received any medications or supplements for at least 1 month before the study.All participants(or their parents if they were under 18)were fully informed about the protocol before the start of the study and gave a written informed consent.The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Ethical Committee of the Faculty of Medical Sciences,University of Kragujevac.
2.2.Protocol
The study started immediately after regular competition season with the first MPET and lasted 4 weeks terminating with the second MPET.During this period,players were subjected to preparatory training in a closed campus in Serbia and they all had the same diet.The regular regime before the study included training once a day for 1.5 h,as a combination of aerobic, conditioning,and strength exercise.The campus regime included 2 training sessions per day,lasting a total of 3 h,with the same combination of exercises,but of higher intensity.
The research protocol started in the morning,between 8:00 a.m.and 9:00 a.m.,after overnight rest and fast.A blood sample was taken from each subject’s antecubital vein and a small catheter was inserted for further blood sampling.A routine medical examination was performed to con firm that all participants were healthy and without any acute or chronic diseases.A study protocol was carefully explained to each of them.Handball players were subjected to the same dietary protocol 3 days before the study.During those 3 days,they were asked to keep a diary of daily food intake.According to their data and the food composition database of the Italian National Institute of Nutrition,the average dietary intake was calculated. Athletes were instructed to avoid any heavy physical activity 24 h before the research and the consumption of alcohol and caffeine 48 h before the test,as well as not to have breakfast before the examination.
The exercise was performed in continuation on a treadmill (Pulsar4.0HPCosmosSports&Medical,Nussdorf-Traunstein,Germany).The starting velocity for the maximal test was the one at which subjects reached the heart rate of 150 beat/min during the 15 min warm-up period.The workload was increased by 2 km/h every 3 min with constant elevation of 3%.24This type of protocol was chosen to reachVO2maxaccord-ing to the following criteria:(a)the heart beat rate equal or greater than the age-predicted maximal value calculated according to the standard formula(220−age,beat/min),(b)the lactate peak higher than 9 mmol/L,and(c)the respiratory exchange ratio(RER)value higher than 1.10.This protocol was validated as appropriate for the handball players.25
The pulmonary oxygen consumption(VO2),CO2production (VCO2),and the expired minute ventilation(VE)were measured continuously using an automated metabolic cart(Quark b2;CosmedSrl,Rome,Italy).The ambient conditions were recorded before each test and the gas analyzer and the flow meter were calibrated with high precision.During sub-maximal and maximal exercise,theVO2values were recorded as average measures for 15 s.The participants were asked to express their subjective feeling of exhaustion by using Borg’s CR10 exhaustion scale.26The heart beat rate was monitored continuously and recorded as average measures for 15 s using a Polar SportTester (Polar Team2 System,Polar Electro Oy,Finland).
2.3.Serum samples
Three samples were obtained at the start of the study and the other 3 after 4 weeks of preparatory training.Blood was drawn: (1)immediately before the test(basal),(2)at the end of the test after reaching the point ofVO2max,and(3)after a 10 min recovery(without eating).VO2maxwas reached at the moment when the increase in workload could not further increase VO2.24Serum samples were prepared from blood by centrifugation at 1500 g for 5 min and stored at−20°C until analysis.
2.4.Determination of insulin and IGF-1 concentrations
Concentrations of insulin and IGF-1 in serum were measured using the commercial immunodiagnostic assays:INSRIA and IGF-1-RIA(INEP,Belgrade,Serbia).
2.5.Determination of relative amounts of IGFBP-1, IGFBP-2,IGFBP-3,and IGFBP-4 by immunoblotting
Electrophoresis under non-reducing conditions(SDS-PAGE, 12%gel)and immunoblotting with polyclonal anti-IGFBP-1, -IGFBP-2,-IGFBP-3,or-IGFBP-4 antibody(Santa Cruz Biotechnology,Santa Cruz,CA,USA)was used for IGFBP detection in serum.27Appropriate Horseradish peroxidase(HRP)-conjugated horse anti-goat secondary antibody was applied (Biosource,Camarillo,CA,USA)and the chemiluminescent substrate(Pierce,Minneapolis,MN,USA).Densitometric analysis of protein bands on immunoblots was done using Image Master Total Lab Version 2.01 software(Amersham BioSciences,Buckinghamshire,UK).
2.6.Statistical data analysis
Anthropometricparametersandconcentrationswere expressed as mean±SD and statistically analyzed by SPSS Version 16.0(SPSS Inc.,Chicago,IL,USA).Relative amounts of IGFBP obtained by densitometry were also expressed as mean±SD.Since all variables showed normal distribution,as checked by the Shapiro–Wilk test,differences between groupswere assessed by the repeated measures ANOVA followed by Tukey post hoc test(p<0.05).

Table 1 Anthropometric characteristics of handball players before and after preparatory training(mean±SD).
3.Results
3.1.Alterations in insulin and IGF-1 levels
Ordinary biochemical and hematological parameters(i.e., concentrations of glucose,urea,creatinine,bilirubin,cholesterol,triglycerides,total proteins,albumin,iron,calcium, hemoglobin,activities of transaminases and alkaline phosphatase,blood cells counts)at the start and at the end of the study for each player were very similar(data not shown).Anthropometric parameters of the players are shown in Table 1 and no signi ficant changes were found between 2 training regimes.
The results on insulin,IGF-1,and IGFBPs were analyzed by comparing values obtained in MPET on treadmill before and after training on campus(Table 2).During MPET on treadmill, concentration of insulin decreased at VO2maxcompared to basalvalue and recovered afterwards(p=0.019 and p=0.021 in the test performed before and after preparatory training,respectively).Concentrations of insulin before the test and after recovery were similar regardless of the training regime.The concentration of insulin at the moment ofVO2max,however,was higher in players after more intensive training on campus (p=0.049).Concentrations of IGF-1 were similar before the test and at VO2maxin both training regimes.IGF-1 level was slightly lower at VO2maxand remained almost unchanged after recovery in regularly exercising players,whereas it raised in playerstrainedoncampus(althoughnotstatistically signi ficantly).
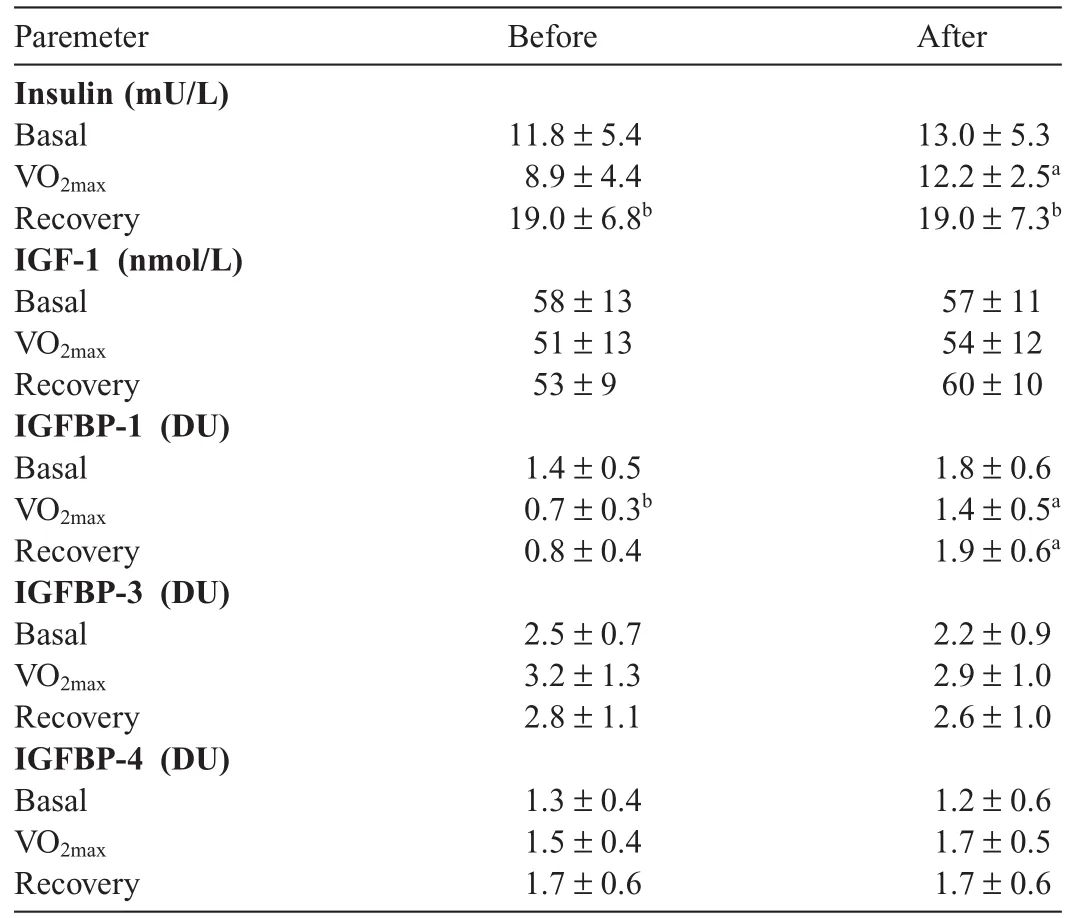
Table 2 ConcentrationsofinsulinandIGF-1,andrelativeamountsofIGFBP-1,-3,and-4 in handball players subjected to strength load test(MPET)before and after preparatory training(mean±SD).
3.2.Alterations in IGFBP levels
The relative amounts of IGFBPs changed as shown in Fig.1. Representative pro files for 6 samples obtained from the same person are given(1–3 before and 4–6 after preparatory training).Densitometric evaluation of protein bands was performed and statistically signi ficant changes were seen only for IGFBP-1 when the entire population was analyzed.Results for IGFBP-1,-3,and-4 expressed in densitometric units(DU)are given in Table 2.The level of IGFBP-1 decreased at VO2maxin either case of training,but signi ficant only in the test performed before preparatory training(p=0.020).The level of IGFBP-1 remained signi ficantly higher in the test performed after the campus regime,both at the VO2maxsampling point(p=0.029) and after the recovery(p=0.023).The level of IGFBP-2 did not seem to be affected by MPET or the exercise mode(data not shown).The concentration of IGFBP-3 was the highest at VO2maxand remained higher at recovery point for both tests compared to the appropriate basal level.The training regime did not affect the pro file of IGFBP-3.Finally,IGFBP-4 exhibited either no change during the test or slight increase at VO2max.
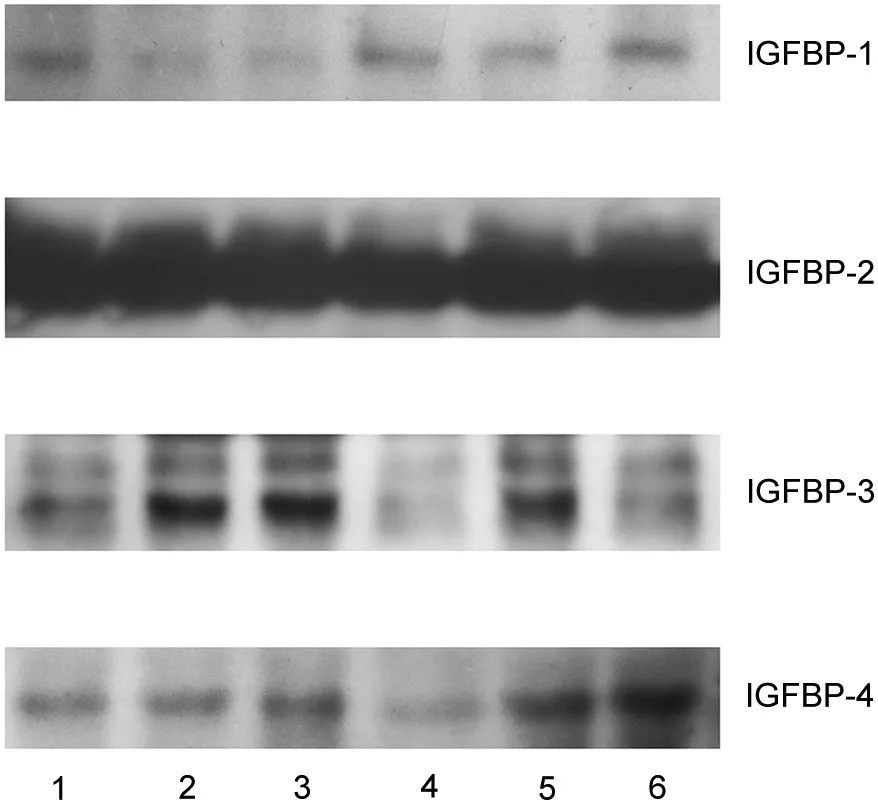
Fig.1.Insulin-like growth factor-binding protein(IGFBP)immunoblotting of 6 serum samples obtained from 1 individual,during 2 maximal progressive exercise tests on treadmill:1 before preparatory training(Samples 1–3)and 1 after(Samples 4–6);Samples 1 and 4 were obtained before MPET,Samples 2 and 5 during MPET at VO2max,Samples 3 and 6 at 10 min after MPET.MPET =maximal progressive exercise tests.
4.Discussion
The general feature of MPET on treadmill performed by the female active handball players was a signi ficant reduction in the levels of insulin and IGFBP-1 at VO2max.After preparatory training however,athletes demonstrated a less pronounced decrease in these parameters at VO2max,compared to regular training.A reduction in insulin level after endurance exercise was reported earlier,28but there are no data on the changes in the IGFBP-1 level at the point of VO2max.
During regular metabolism,concentrations of insulin and IGFBP-1 are inversely proportional,as insulin is one of the regulators(suppressor)of IGFBP-1 synthesis in the liver.29Response of the liver to insulin,however,needs time.In oral glucose tolerance test,a decrease in the concentration of IGFBP-1 was found to occur 1 h after the rise in the concentration of insulin.30Thus,in the case of MPET,which lasted approximately 15 min,the complete feedback control between insulin and IGFBP-1 could not be established.The more likely explanation for the simultaneous decrease in the concentrations of insulin and IGFBP-1 is the response to stress,which involved activation of pro-in flammatory mechanisms.Since MPET lasted a relatively short period of time,reduced concentrations of the investigated parameters most likely resulted from the increased activity of proteases and other stress-related degradation mechanisms.It was already documented that intensive training up-regulates expression and release of proteolytic enzymes capable of degrading IGFBP-1.31IGFBP-1 in the circulation predominantly inhibits the activity of IGF-1 and the concentration of free IGF-1 seems to be primarily determined by the IGFBP-1 level.32Reduced IGFBP-1 at VO2maxmay be seen as a mechanism to redistribute IGF-1 possibly enabling it to perform insulin-like activity and assist in intra-cellular glucose transportation.
The inverse correlation between insulin and IGFBP-1 was lost during MPET.Results of this study may be interpreted as less severe stress-induced depression of insulin and IGFBP-1 after preparatory training.But another metabolic mechanism cannot be excluded,and that is potentially impaired insulin sensitivity resulting in higher level of IGFBP-1.Less pronounced changes of insulin and IGFBP-1 atVO2maxmay be also connected with increased expression of insulin receptors due to training.33Studies using biopsies could possibly help,but the approach is not readily applicable on human subjects.Muscle mass and mRNA levels for some growth factors were found reduced in patients on maintenance hemodialysis.34When patients were subjected to endurance exercise,the increase in muscle mRNA levels for some IGFBPs was noted,but IGFBP-1 mRNA was undetectable.34It may be hypothesized that adjustments in the insulin/IGFBP-1 relationship primarily occur in the liver,yet further studies are needed to resolve differential effects(and possible consequences)of regular and preparatory training.
The limitation of this study was the lack of data on the hormonal status of the participants at the moment of testing and the fact that they were not in the same phase of menstrual cycle. It was shown recently that a decreased progesterone/estradiolratio may induce a slight increase in insulin levels,thus possibly affecting metabolic pathways dependent on insulin.35
There is little information available on the exercise-induced simultaneous adaptation of the musculoskeletal and endocrine system,especially in adolescents and young athletes,which is surprising considering the importance of that population.The lack of information on biochemical responses to exercise in young individuals can be attributed to ethical concerns which limit invasive research in children and adolescents.36The data collected in this study and future investigations on the traininginduced changes in the insulin/IGF/IGFBP axis could be helpful in preventing overtraining,fatigue,and muscular damage.36The evaluation of the speci fic biochemical pathways is necessary to resolve whether the adaptive potential of speci fic endocrine components is suf ficient to protect athletes from the muscular damage and glycogen depletion leading to decreased physical performance.
Taking into account the nature of handball as a game(relatively small playing field,only 6 players,with very dynamic actions during short periods of time),hormonal changes in MPET on treadmill can be extrapolated to a real situation such as very intensive periods of the game during an ordinary match. Thus,changes that were recorded in this study may be expected to occur regularly in handball professionals.Although preparatory training seems bene ficial by enabling smoother insulin/ IGFBP-1 alterations upon physical overload,the trend in changes during MPET(and,possibly,during periods of the intensive game)suggests disturbed feedback control.Therefore,one can wonder whether frequent episodes of this type may induce long-lasting metabolic consequences,one of them being reduced insulin sensitivity.It would also be interesting to determine,over the period of a few years,insulin/IGFBP-1 relation during MPET change,as well as the general insulin sensitivity,in the investigated handball players.Finally,it would be interesting to investigate whether similar outcomes can be recorded for other athletes(female/male)involved in similar or completely different type of sports.
Acknowledgment
This work was supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia(No.173042 and III41030).
Authors’contributions
ON participated in the study design,laboratory tests and data analysis,and drafted the manuscript;MŠ and GM performed laboratory tests;ZV and VJ monitored and supervised MPET test and sample collection;MG participated in data analysis;VV participated in the study design,data analysis and helped to draft the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
1.Plasqui G,Westerterp KR.Physical activity and insulin resistance.Curr Nutr Food Sci 2007;3:157–60.
2.Godfrey RJ,Madgwick Z,Whyte GP.The exercise-induced growth hormone response in athletes.Sports Med 2003;33:599–613.
3.Sacheck JM,Ohtsuka A,McLary SC,Goldberg AL.IGF-I stimulates muscle growth by suppressing protein breakdown and expression of atrophy-related ubiquitin ligases,atrogin-1 and MuRF1.Am J Physiol Endocrinol Metab 2004;287:E591–601.
4.SonksenPH.Insulin,growthhormoneandsport.JEndocrinol 2001;170:13–25.
5.Krebs HA,Weitzman PDJ.Krebs’citric acid cycle:half a century and still turning.London:Biochemical Society;1987.
6.Cryer PE.Glucose counterregulation:prevention and correction of hypoglycemiainhumans.AmJPhysiolEndocrinolMetab 1993;264:E149–55.
7.Ballard TLP,Clapper JA,Specker BL,Binkley TL,Vukovich MD.Effect of protein supplementation during a 6-mo strength and conditioning program on insulin-like growth factor I and markers of bone turnover in young adults.Am J Clin Nutr 2005;81:1442–8.
8.Borst SE,De Hoyos DV,Garzarella L,Vincent K,Pollock BH,Lowenthal DT,et al.Effects of resistance training on insulin-like growth factor-I and IGF binding proteins.Med Sci Sports Exerc 2001;33:648–53.
9.Gregory SM,Spiering BA,Alemany JA,Tuckow AP,Rarick KR,Staab JS, et al.Exercise-induced insulin-like growth factor I system concentrations after training in women.Med Sci Sports Exerc 2013;45:420–8.
10.Koziris LP,Hickson RC,Chatterton Jr RT,Groseth RT,Christie JM, God flies DG,et al.Serum levels of total and free IGF-I and IGFBP-3 are increasedandmaintainedinlong-termtraining.J ApplPhysiol 1999;86:1436–42.
11.Nindl BC,McClung JP,Miller JK,Karl JP,Pierce JR,Sco field DE,et al. Bioavailable IGF-I is associated with fat-free mass gains after physical training in women.Med Sci Sports Exerc 2011;43:793–9.
12.Rezaee S,Kahrizi S,Hedayati M.Hormonal response of combining endurance-resistance exercise in healthy young men.J Sports Med Phys Fitness 2014;54:244–51.
13.Tsai CL,Wang CH,Pan CY,Chen FC,Huang TH,Chou FY.Executive function and endocrinological response to acute resistance exercise.Front Behav Neurosci 2014;8:262.doi:10.3389/fnbeh.2014.00262
14.Vinogradova OL,Popov DV,Netreba AI,Tsvirkun DV,Kurochkina NS, Bachinin AV,et al.Optimization of training:new developments in safe strength training.Hum Physiol 2013;39:511–23.
15.Eliakim A,Nemet D,Bar-Sela S,Higer Y,Falk B.Changes in circulating IGF-I and their correlation with self-assessment and fitness among elite athletes.Int J Sports Med 2002;23:600–3.
16.Schmitz KH,Ahmed RL,Yee D.Effects of a 9-month strength training intervention on insulin,insulin-like growth factor(IGF)-I,IGF-binding protein(IGFBP)-1 and IGFBP-3 in 30–50-year-old women.Cancer Epidemiol Biomarkers Prev 2002;11:1597–604.
17.Eliakim A,Portal S,Zadik Z,Meckel Y,Nemet D.Training reduces catabolic and in flammatory response to a single practice in female volleyball players.J Strength Cond Res 2013;27:3110–5.
18.Meckel Y,Eliakim A,Seraev M,Zaldivar F,Cooper DM,Sagiv M,et al. The effect of a brief sprint interval exercise on growth factors and in flammatory mediators.J Strength Cond Res 2009;23:225–30.
19.Nindl BC,Alemany JA,Tuckow AP,Rarick KR,Staab JS,Kraemer WJ, et al.Circulating bioactive and immunoreactive IGF-I remain stable in women,despite physical fitness improvements after 8 weeks of resistance, aerobic,and combined exercise training.J Appl Physiol 2010;109:112–20.
20.Koistinen H,Koistinen R,Selenius L,Ylikorkala O,Seppälä M.Effect of marathon run on serum IGF-I and IGF-binding protein 1 and 3 levels.J Appl Physiol 1996;80:760–4.
21.Geyer R,Predel HG,Wolber T,Mellwig KP,Schmied C.Pre-competition cardiac screening in professional handball players—setting up at the EHF European Handball Championship 2010 inAustria.Wien MedWochenschr 2011;161:387–93.
22.Massuca LM,Fragoso I,Teles J.Attributes of top elite team-handball players.J Strength Cond Res 2014;28:178–86.
23.Armstrong N.Young people are fit and active—fact or fiction?J Sport Health Sci 2012;1:131–40.
24.Howley ET,Bassett Jr DR,Welch HG.Criteria for maximal oxygen uptake:review and commentary.Med Sci Sports Exerc 1995;27:1292–301.
25.Cubrilo D,Djordjevic D,Zivkovic V,Djuric D,Blagojevic D,Spasic M, et al.Oxidative stress and nitrite dynamics under maximal load in elite athletes:relation to sport type.Mol Cell Biochem 2011;355:273–9.
26.Borg GA.Psychophysical bases of perceived exertion.Med Sci Sports Exerc 1982;14:377–81.
27.Hossenlopp P,Seurin D,Segovia-Quinson B,Binoux M.Identi fication of an insulin-like growth factor binding protein in human cerebrospinal fluid with a selective af finity for IGF-II.FEBS Lett 1986;208:439–44.
28.Stokes KA,Gilbert KL,Hall GM,Andrews RC,Thompson D.Different responses of selected hormones to three types of exercise in young men. Eur J Appl Physiol 2013;113:775–83.
29.Brismar K,Fernqvist-Forbes E,Wahren J,Hall K.Effect of insulin on the hepatic production of insulin-like growth factor binding protein-1 (IGFBP-1),IGFBP-3 and IGF-I in insulin-dependent diabetes.J Clin Endocrinol Metab 1994;79:892–8.
30.Nedic´O,Masnikosa R.The change in the insulin-like growth factor binding protein 1 isoform pattern during the course of oral glucose tolerance test.Metab Clin Exp 2008;57:658–61.
31.Coppock HA,White A,Aplin JD,Westwood M.Matrix metalloprotease-3 and-9 proteolyze insulin-like growth factor-binding protein 1.Biol Reprod 2004;71:438–43.
32.Lee PDK,Giudice LC,Conover CA,Powell DR.Insulin-like growth factor binding protein-1:recent findings and new directions.Proc Soc Exp Biol Med 1997;16:319–57.
33.Lakhdar N,Bouassida A,Saad HB,Zaouali M,Zbidi A,Tabka Z.Effect of trainingstatusonadiponectinconcentrations.SportSciHealth 2009;5:113–9.
34.Kopple JD,Cohen AH,Wang H,Qing D,Tang Z,Fournier M,et al.Effect of exercise on mRNA levels for growth factors in skeletal muscle of hemodialysis patients.J Ren Nutr 2006;16:312–24.
35.Yildir IC,Kutluturk F,Tasliyurt T,Yelken BM,Acu B,Beyhan M,et al. Insulin resistance and cardiovascular risk factors in women with PCOS whohavenormalglucosetolerancetest.GynecolEndocrinol 2013;29:148–51.
36.Djordjevic D,Cubrilo D,Macura M,Barudzic N,Djuric D,Jakovljevic V. The in fluence of training status on oxidative stress in young male handball players.Mol Cell Biochem 2011;351:251–9.
30 March 2015;revised 3 July 2015;accepted 10 October 2015
Available online 21 January 2016
Peer review under responsibility of Shanghai University of Sport.
*Corresponding author.
E-mail address:olgica@inep.co.rs(O.Nedic´)
http://dx.doi.org/10.1016/j.jshs.2016.01.014
2095-2546/©2017 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
 Journal of Sport and Health Science2017年3期
Journal of Sport and Health Science2017年3期
- Journal of Sport and Health Science的其它文章
- Time for a paradigm shift in the classi fication of muscle injuries
- Rehabilitation and return to sport after hamstring strain injury
- Risk factors for hamstring injuries in Australian male professional cricket players
- Relationships among hamstring muscle optimal length and hamstring flexibility and strength
- The effect of hamstring flexibility on peak hamstring muscle strain in sprinting
- Motivation dimensions for running a marathon:A new model emerging from the Motivation of Marathon Scale(MOMS)