不同运动方式改善心力衰竭病人心肺功能的贝叶斯网状Meta分析
2024-03-22 12:04耑亚静李晓虹闫晓丹许佳星
中西医结合心脑血管病杂志 2024年1期
耑亚静 李晓虹 闫晓丹 许佳星
摘要 目的:评价不同运动方式改善心力衰竭病人心肺功能的效果,为心力衰竭病人心脏康复提供参考。方法:检索国内外数据库中关于运动改善心力衰竭病人心肺功能的随机对照试验,根据纳入与排除标准筛选文献,使用Rstudio软件GEMTC包调用JAGS进行贝叶斯网状Meta分析。结果:最终纳入37项研究,涉及24种不同运动方式干预措施。贝叶斯网状 Meta分析结果显示,与不运动、极低吸气肌运动相比,高强度连续抗阻运动、高强度连续有氧运动、高强度连续抗阻运动+高强度连续有氧运动、高强度间歇有氧运动+高强度间歇阻抗运动、中等强度连续有氧运动、高强度间歇有氧运动、高强度间歇阻抗运动、中等连续有氧运动+中强度连续阻抗运动+高强度吸气肌运动、低强度吸气肌运动均可改善心力衰竭病人心肺功能,差异有统计学意义(P<0.05)。贝叶斯有效率排序结果显示,24种运动方式改善心力衰竭病人心肺功能效果居前3位的是高强度间歇有氧运动、高强度间歇有氧运动+高强度间歇阻抗运动、中等连续有氧运动+中强度连续阻抗运动+高强度吸气肌运动。结论:现有证据表明,心力衰竭病人积极参加运动训练可以改善心肺功能、运动能力。高强度间歇有氧运动对改善峰值耗氧量最有效果,但是不同间歇方式是否有差异需要进一步研究。
关键词 心力衰竭;运动康复;峰值耗氧量;网状Meta分析
doi:10.12102/j.issn.1672-1349.2024.01.026
心力衰竭(HF)是心血管疾病的终末阶段,全球每年大约有65万新发病例,给许多国家造成了重大的医疗负担[1]。心力衰竭病人通常不能保持稳定的心功能,因此需要持续的医疗管理和间歇性的住院治疗。在美国,心力衰竭護理的总费用每年超过400亿美元,其中50%以上用于住院治疗[2-3]。此外,随着全球人口老龄化,预计未来几十年心力衰竭的发病率呈增长趋势[4]。运动训练有益于心力衰竭病人的运动能力、预后、生活质量和心脏功能等。衡量运动能力的金标准是在心肺运动测试(CPET)中对峰值耗氧量(peak VO2)的直接心肺评估[5]。《慢性稳定性心力衰竭运动康复中国专家共识》[6]指出,对于不同的慢性心力衰竭人群,采用不同运动强度、间歇或者连续效果是否不同?如何组合有氧运动和抗阻运动与吸气肌训练效果最佳?其他运动如瑜伽、舞蹈、水疗等对心力衰竭病人运动能力的影响,均有待进一步研究。为此,本研究采用网状Meta分析不同运动训练干预后peak VO2的变化,为心力衰竭病人心脏康复提供参考。
1 资料与方法
1.1 检索策略
按照系统审查和综合分析(PRISMA)报告首选报告项目的指导方针编辑。结合医学主题词(MeSH)和关键词来描述病人群体、干预和结果(改编的PICO搜索)。索引词不同的情况下,对每个数据库的搜索策略进行修改,插入其他未报告的关键词和网格词。对多个数据库(PubMed、the Cochrane Library、Web of Science、CINAHL护理学数据库、万方数据库、中国生物医学文献数据库、中国知网)进行系统检索,检索时限为建库至2022年7月1日。
1.2 纳入与排除标准
纳入标准:1)研究对象为心力衰竭病人;2)病人年龄≥18岁;3)结局指标包含peak VO2;4)比较两种不同的训练模式;5)研究以英文、中文发表;6)研究设计为随机对照试验(RCT)。排除标准:1)不以固定方式给予运动干预;2)心脏移植;3)收集了正在进行的(未发表的)研究或其他相关数据的专家意见和建议。
1.3 文献筛选及资料提取
利用EndNote将重复的研究删除,由2名研究人员根据选择标准对全文进行检索和评价,意见不一致时与第3名研究人员协商讨论。仔细阅读纳入文献,将资料提取填入预先制定的资料提取表中,资料提取内容包括:1)研究者的基本情况,如第一作者的姓名;2)两组病人的基线资料[研究对象心功能、年龄、性别比例、体质指数(BMI)等];3)样本量与干预措施。
1.4 纳入研究的偏倚风险评价
依照Cochrane手册5.1.0版中建议用偏倚风险评估工具进行文献质量评价。评价内容包括:随机分组的产生方法,分配隐藏的实施,参与者、研究者及结果测评者盲法,结局指标的完整性,选择性报告,其他偏倚等,每项以“低风险偏倚”“不清楚”“高风险偏倚”来评价。评价等级分为3级,所有条目评估结果为“低风险偏倚”则其发生偏倚的可能性极低,只要由条目评估结果为“高风险偏倚”则其发生偏倚的可能性极高,部分满足上述条目,则发生偏倚的风险可能性为中等。
1.5 统计学处理
运用Rstudio调用GEMTC包进行统计分析,由于纳入的是RCT研究,因此提取干预前后差值的均值和标准差。因为所有的值都是以相同的单位报告的,所以效应大小为原始平均差异。用RevMan软件对提取的数据进行直接Meta分析。用R软件对提取的数据进行网状Meta分析,并制作网状关系图、森林图、收敛诊断图、排序图同时制作赛联表。使用先验选择的随机效应模型进行Meta分析,以评估研究中是否存在异质性,用I2值判断研究的异质性大小,I2≤50%,则认为纳入研究异质性可接受,采用固定效应模型,当I2>50%,则认为有统计学异质性,采用随机效应模型进行分析。采用节点分离法进行不一致性检验,当P<0.05说明直接比较与间接比较不一致,用不一致模型进行分析,当P>0.05采用一致性模型进行分析。贝叶斯网状Meta分析参数设置为马尔可夫蒙特卡洛MCMC的链条数为4,退火次数为20 000次,迭代次数为50 000次。通过潜在尺度减少因子(potential scale reduced factor,PSRF)判断迭代效果的收敛性,当潜在尺度减少因子值接近或者等于1时,收敛完全,表示该模型稳定性良好,可进行数据分析。
2 结 果
2.1 文献检索结果
共检出相关文献957篇,根据纳入及排除标准,最后纳入符合条件的文献37篇[7-43]。
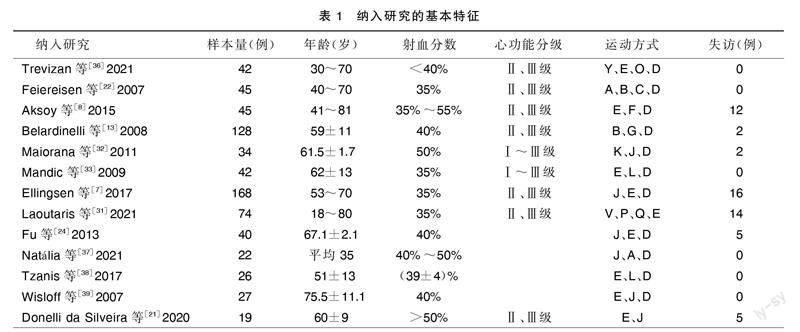
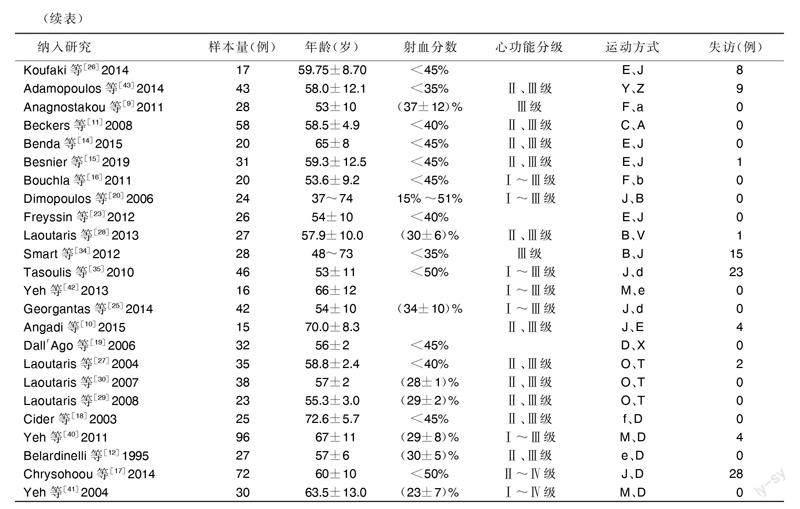
2.2 纳入研究的基本特征
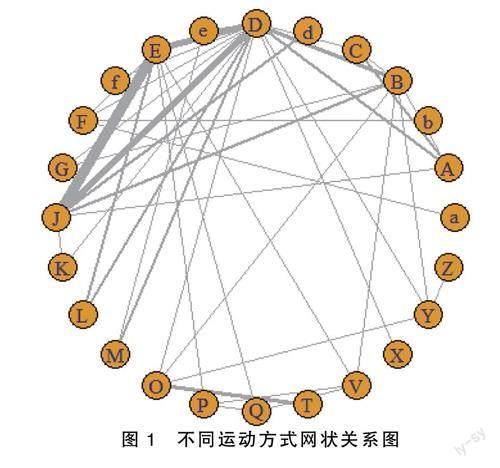
共纳入37篇文献,涉及24项运动方式干预措施,心力衰竭病人心肺运动测试中对peak VO2影响的网状关系见图1,纳入研究的基本特征见表1。图1及表1运动方式中:A代表高强度连续抗阻运动;B代表高强度连续有氧运动;C代表高强度连续抗阻运动+高强度连续有氧运动;D代表无运动对照;E代表中等强度连续有氧运动;F代表中等强度间歇有氧运动;G代表新式华尔兹;H代表极低强度吸气肌运动+中强度连续阻抗运动;I代表低强度吸气肌运动+中强度连续阻抗运动;J代表高強度间歇有氧运动;K代表高强度间歇阻抗运动;L代表中等连续有氧运动+中强度连续阻抗运动;M代表太极拳;O代表高强度吸气肌运动;P代表高强度吸气肌运动+中等连续有氧运动;Q代表中等连续有氧运动+中强度连续阻抗运动;T代表极低吸气肌运动;V代表中等连续有氧运动+中强度连续阻抗运动+高强度吸气肌运动;X代表低强度吸气肌运动;Y代表高强度连续有氧运动+高强度吸气肌运动;Z代表高强度连续有氧运动+假性吸气肌运动;a代表中等强度间歇有氧运动+高强度连续抗阻运动;b代表中等强度间歇有氧运动+中强度连续抗阻运动;d代表高强度间歇有氧运动+高强度间歇阻抗运动;e代表低至中强度连续有氧运动;f代表水疗。
2.3 纳入文献的方法学质量评价
根据JBI2015版RCT文献质量表评价要求,对纳入的各项研究进行质量评价,并应用RevMan 5.4呈现主要结局指标文献评价结果。详见图2。
2.4 Meta分析结果
2.4.1 异质性检验
有5项研究比较了中等强度连续有氧运动与高强度间歇有氧运动后peak VO2的变化。Meta分析显示支持中等强度连续有氧运动的总体加权平均原始差值为-1.94 mL/(kg·min),95%CI(-3.40,-0.48),异质性较小(P=0.99,I2=0%),高强度间歇有氧运动对于改善心力衰竭病人的运动能力优于中等强度连续有氧运动。有3项研究比较了高强度吸气肌运动与极低吸气肌运动后peak VO2的变化。Meta分析结果显示,支持高强度吸气肌运动的总体加权平均原始差值为2.66 mL/(kg·min),95%CI(2.23,3.09),异质性较小(P=0.36,I2=3%),高强度吸气肌运动对于改善心力衰竭病人的运动能力优于极低吸气肌运动。
2.4.2 不一致性检测与模型收敛性诊断
经不一致模型检验P>0.05,所以拟使用一致性模型进行分析。因网状关系存在多个闭合环,所以进行环的不一致性检测,利用节点分离法探讨模型的局部不一致性,结果P>0.05,提示闭合环一致性良好,即直接比较与间接比较的结果符合一致性,并且不存在局部不一致的情况,故本研究采用一致性检验。收敛性评估结果显示PSRF值为1.03,收敛完全,表示该模型稳定性良好,可进行数据的分析。
2.4.3 贝叶斯网状Meta分析结果
与D、T比较,A、B、C、d、E、J、K、V、X运动方式均可提高心力衰竭病人心肺功能,差异有统计学意义(P<0.05)。但A、B、C、d、E、J、K、V、X运动后peak VO2比较差异均无统计学意义(P>0.05)。贝叶斯有效率累积排序概率结果显示,24种运动方式改善心力衰竭病人心肺功能效果依次为J、d、V、K、a、b、A、X、c、F、E、P、B、Q、G、f、Z、Y、L、M、O、e、D、T。其中排在前3位的运动方式为J、d、V。详见图3。
3 讨 论
peak VO2是衡量运动能力的客观指标,根据Fick方程,peak VO2为心排血量和动静脉氧差的乘积[44]。其中心排血量和动静脉氧差分别反映对氧气的输送和提取量,心排血量的增加主要是通过心率的增加而实现[45]。高强度间歇有氧运动被认为是保持身体活跃的一种时间效率高的替代策略,指南指出与中到高强度持续运动训练相比,高强度间歇有氧运动峰值peak VO2从1.0 mL/(kg·min)提高到2.14 mL/(kg·min)[46]。网状Meta分析结果排序与指南一致,高强度间歇运动较其他中高强度的持续运动更能提高peak VO2,这可能与高强度间歇有氧运动在很短的时间内施加强度和/或超过最大强度的负荷,运动强度的增加、刺激的持续时间、Ⅰ型和Ⅱ型肌肉纤维的招募/激活以及高能量底物的使用使得peak VO2大幅增加[47]。
本研究存在一定局限性,纳入文献虽提及随机分组,但部分未详细描述随机产生方法,也未进行分配隐藏及盲法,所以纳入的文献方法学质量不高,可能对结果产生一定影响,也未考虑耗材、费用等问题,不能进行成本估计。
4 结 论
心力衰竭病人积极参加运动训练可以改善心肺功能、运动能力,高强度间歇有氧运动对改善peak VO2最有效果,但是不同间歇方式是否有差异需要进一步研究。将来应该进行更多标准化、高质量、严格的(多中心)临床试验,以评估最有效的间歇时间。
参考文献:
[1]ALI D,CALLAN N,ENNIS S,et al.Heart failure with preserved ejection fraction (HFpEF) pathophysiology study (IDENTIFY-HF):does increased arterial stiffness associate with HFpEF,in addition to ageing and vascular effects of comorbidities? Rationale and design[J].BMJ Open,2019,9(11):e027984.
[2]FERNANDEZ C,RYS J,STRM K,et al.Circulating protein biomarkers predict incident hypertensive heart failure independently of N-terminal pro-B-type natriuretic peptide levels[J].ESC Heart Failure,2020,7(4):1891-1899.
[3]BOZKURT B,HERSHBERGER R E,BUTLER J,et al.2021 ACC/AHA key data elements and definitions for heart failure:a report of the American College of Cardiology/American Heart Association task force on clinical data standards(writing committee to develop clinical data standards for heart failure)[J].Circulation Cardiovascular Quality and Outcomes,2021,14(4):e000102.
[4]MCEWAN P,PONIKOWSKI P,DAVIS J A,et al.Ferric carboxymaltose for the treatment of iron deficiency in heart failure:a multinational cost-effectiveness analysis utilising AFFIRM-AHF[J].European Journal of Heart Failure,2021,23(10):1687-1697.
[5]GIANNITSI S,BOUGIAKLI M,BECHLIOULIS A,et al.6-minute walking test:a useful tool in the management of heart failure patients[J].Therapeutic Advances in Cardiovascular Disease,2019,13:1753944719870084.
[6]中國康复医学会心血管病专业委员会,中国老年学学会心脑血管病专业委员会.慢性稳定性心力衰竭运动康复中国专家共识[J].中华心血管病杂志,2014,42(9):714-720.
[7]ELLINGSEN ,HALLE M,CONRAADS V,et al.High-intensity interval training in patients with heart failure with reduced ejection fraction[J].Circulation,2017,135(9):839-849.
[8]AKSOY S,FINDIKOGLU G,ARDIC F,et al.Effect of 10-week supervised moderate-intensity intermittent vs.continuous aerobic exercise programs on vascular adhesion molecules in patients with heart failure[J].American Journal of Physical Medicine & Rehabilitation,2015,94(10 Suppl 1):898-911.
[9]ANAGNOSTAKOU V,CHATZIMICHAIL K,DIMOPOULOS S,et al.Effects of interval cycle training with or without strength training on vascular reactivity in heart failure patients[J].Journal of Cardiac Failure,2011,17(7):585-591.
[10]ANGADI S S,MOOKADAM F,LEE C D,et al.High-intensity interval training vs.moderate-intensity continuous exercise training in heart failure with preserved ejection fraction:a pilot study[J].Journal of Applied Physiology,2015,119(6):753-758.
[11]BECKERS P J,DENOLLET J,POSSEMIERS N M,et al.Combined endurance-resistance training vs.endurance training in patients with chronic heart failure:a prospective randomized study[J].European Heart Journal,2008,29(15):1858-1866.
[12]BELARDINELLI R,GEORGIOU D,SCOCCO V,et al.Low intensity exercise training in patients with chronic heart failure[J].Journal of the American College of Cardiology,1995,26(4):975-982.
[13]BELARDINELLI R,LACALAPRICE F,VENTRELLA C,et al.Waltz dancing in patients with chronic heart failure:new form of exercise training[J].Circulation Heart Failure,2008,1(2):107-114.
[14]BENDA N M,SEEGER J P,STEVENS G G,et al.Effects of high-intensity interval training versus continuous training on physical fitness,cardiovascular function and quality of life in heart failure patients[J].PLoS One,2015,10(10):e0141256.
[15]BESNIER F,LABRUNE M,RICHARD L,et al.Short-term effects of a 3-week interval training program on heart rate variability in chronic heart failure.A randomised controlled trial[J].Annals of Physical and Rehabilitation Medicine,2019,62(5):321-328.
[16]BOUCHLA A,KARATZANOS E,DIMOPOULOS S,et al.The addition of strength training to aerobic interval training:effects on muscle strength and body composition in CHF patients[J].Journal of Cardiopulmonary Rehabilitation and Prevention,2011,31(1):47-51.
[17]CHRYSOHOOU C,TSITSINAKIS G,VOGIATZIS I,et al.High intensity,interval exercise improves quality of life of patients with chronic heart failure:a randomized controlled trial[J].QJM,2014,107(1):25-32.
[18]CIDER A,SCHAUFELBERGER M,SUNNERHAGEN K S,et al.Hydrotherapy--a new approach to improve function in the older patient with chronic heart failure[J].European Journal of Heart Failure,2003,5(4):527-535.
[19]DALL′AGO P,CHIAPPA G R S,GUTHS H,et al.Inspiratory muscle training in patients with heart failure and inspiratory muscle weakness[J].Journal of the American College of Cardiology,2006,47(4):757-763.
[20]DIMOPOULOS S,ANASTASIOU-NANA M,SAKELLARIOU D,et al.Effects of exercise rehabilitation program on heart rate recovery in patients with chronic heart failure[J].European Journal of Cardiovascular Prevention & Rehabilitation,2006,13(1):67-73.
[21]DONELLI DA SILVEIRA A,BEUST DE LIMA J,DA SILVA PIARDI D,et al.High-intensity interval training is effective and superior to moderate continuous training in patients with heart failure with preserved ejection fraction:a randomized clinical trial[J].European Journal of Preventive Cardiology,2020,27(16):1733-1743.
[22]FEIEREISEN P,DELAGARDELLE C,VAILLANT M,et al.Is strength training the more efficient training modality in chronic heart failure?[J].Medicine and Science in Sports and Exercise,2007,39(11):1910-1917.
[23]FREYSSIN C,VERKINDT C,PRIEUR F,et al.Cardiac rehabilitation in chronic heart failure:effect of an 8-week,high-intensity interval training versus continuous training[J].Archives of Physical Medicine and Rehabilitation,2012,93(8):1359-1364.
[24]FU T C,WANG C H,LIN P S,et al.Aerobic interval training improves oxygen uptake efficiency by enhancing cerebral and muscular hemodynamics in patients with heart failure[J].International Journal of Cardiology,2013,167(1):41-50.
[25]GEORGANTAS A,DIMOPOULOS S,TASOULIS A,et al.Beneficial effects of combined exercise training on early recovery cardiopulmonary exercise testing indices in patients with chronic heart failure[J].Journal of Cardiopulmonary Rehabilitation and Prevention,2014,34(6):378-385.
[26]KOUFAKI P,MERCER T H,GEORGE K P,et al.Low-volume high-intensity interval training vs continuous aerobic cycling in patients with chronic heart failure:a pragmatic randomised clinical trial of feasibility and effectiveness[J].Journal of Rehabilitation Medicine,2014,46(4):348-356.
[27]LAOUTARIS I,DRITSAS A,BROWN M D,et al.Inspiratory muscle training using an incremental endurance test alleviates dyspnea and improves functional status in patients with chronic heart failure[J].European Journal of Cardiovascular Prevention & Rehabilitation,2004,11(6):489-496.
[28]LAOUTARIS I D,ADAMOPOULOS S,MANGINAS A,et al.Benefits of combined aerobic/resistance/inspiratory training in patients with chronic heart failure.A complete exercise model? A prospective randomised study[J].International Journal of Cardiology,2013,167(5):1967-1972.
[29]LAOUTARIS I D,DRITSAS A,BROWN M D,et al.Effects of inspiratory muscle training on autonomic activity,endothelial vasodilator function,and N-terminal pro-brain natriuretic peptide levels in chronic heart failure[J].Journal of Cardiopulmonary Rehabilitation and Prevention,2008,28(2):99-106.
[30]LAOUTARIS I,DRITSAS A,ADAMOPOULOS S,et al Immune response to inspiratory muscle training in patients with chronic heart failure[J].Eur J Cardiovasc Prev Rehabil,2007,14:679-685.
[31]LAOUTARIS I D,PIOTROWICZ E,KALLISTRATOS M S,et al.Combined aerobic/resistance/inspiratory muscle training as the optimum exercise programme for patients with chronic heart failure:ARISTOS-HF randomized clinical trial[J].European Journal of Preventive Cardiology,2021,28(15):1626-1635.
[32]MAIORANA A J,NAYLOR L H,EXTERKATE A,et al.The impact of exercise training on conduit artery wall thickness and remodeling in chronic heart failure patients[J].Hypertension,2011,57(1):56-62.
[33]MANDIC S,TYMCHAK W,KIM D,et al.Effects of aerobic or aerobic and resistance training on cardiorespiratory and skeletal muscle function in heart failure:a randomized controlled pilot trial[J].Clinical Rehabilitation,2009,23(3):207-216.
[34]SMART N A,STEELE M.A comparison of 16 weeks of continuous vs intermittent exercise training in chronic heart failure patients[J].Congestive Heart Failure,2012,18(4):205-211.
[35]TASOULIS A,PAPAZACHOU O,DIMOPOULOS S,et al.Effects of interval exercise training on respiratory drive in patients with chronic heart failure[J].Respiratory Medicine,2010,104(10):1557-1565.
[36]TREVIZAN P F,ANTUNES-CORREA L M,LOBO D M L,et al.Effects of inspiratory muscle training combined with aerobic exercise training on neurovascular control in chronic heart failure patients[J].ESC Heart Failure,2021,8(5):3845-3854.
[37]NATLIA T,AMANDA V,KENNETH V,et al.High-intensity interval training versus progressive high-intensity circuit resistance training on endothelial function and cardiorespiratory fitness in heart failure:a preliminary randomized controlled trial[J].PLoS One,2021,16(10):e0257607.
[38]TZANIS G,PHILIPPOU A,KARATZANOS E,et al.Effects of high-intensity interval exercise training on skeletal myopathy of chronic heart failure[J].Journal of Cardiac Failure,2017,23(1):36-46.
[39]WISLOFF U,STOYLEN A,LOENNECHEN J P,et al.Superior cardiovascular effect of aerobic interval-training versus moderate continuous training in elderly heart failure patients[J].Medicine & Science in Sports & Exercise,2007,39(5):S32.
[40]YEH G Y,MCCARTHY E P,WAYNE P M,et al.Tai Chi exercise in patients with chronic heart failure:a randomized clinical trial[J].Archives of Internal Medicine,2011,171(8):750-757.
[41]YEH G Y,WOOD M J,LORELL B H,et al.Effects of Tai Chi mind-body movement therapy on functional status and exercise capacity in patients with chronic heart failure:a randomized controlled trial[J].The American Journal of Medicine,2004,117(8):541-548.
[42]YEH G Y,WOOD M J,WAYNE P M,et al.Tai Chi in patients with heart failure with preserved ejection fraction[J].Congestive Heart Failure,2013,19(2):77-84.
[43]ADAMOPOULOS S,SCHMID J P,DENDALE P,et al.Combined aerobic/inspiratory muscle training vs.aerobic training in patients with chronic heart failure:the Vent-HeFT trial:a European prospective multicentre randomized trial[J].European Journal of Heart Failure,2014,16(5):574-582.
[44]KITZMAN D W.Understanding results of trials in heart failure with preserved ejection fraction[J].Journal of the American College of Cardiology,2011,57(16):1687-1689.
[45]MONTERO D,DIAZ-CAESTRO C.Determinants of exercise intolerance in heart failure with preserved ejection fraction:a systematic review and Meta-analysis[J].International Journal of Cardiology,2018,254:224-229.
[46]SHOEMAKER M J,DIAS K J,LEFEBVRE K M,et al.Physical therapist clinical practice guideline for the management of individuals with heart failure[J].Physical Therapy,2020,100(1):14-43.
[47]ATAKAN M M,LI Y C,KO瘙塁AR瘙塁N,et al.Evidence-based effects of high-intensity interval training on exercise capacity and health:a review with historical perspective[J].International Journal of Environmental Research and Public Health,2021,18(13):7201.
(收稿日期:2022-09-04)
(本文編辑郭怀印)
基金项目 保定市科技计划项目(No.2241ZF064)
通讯作者 李晓虹,E-mail:2787811317@qq.com
引用信息 耑亚静,李晓虹,闫晓丹,等.不同运动方式改善心力衰竭病人心肺功能的贝叶斯网状Meta分析[J].中西医结合心脑血管病杂志,2024,22(1):138-143.
猜你喜欢
科教导刊·电子版(2017年5期)2017-04-01
中国现代医生(2016年32期)2017-03-02
中国实用医药(2016年27期)2016-11-30
中外医学研究(2016年28期)2016-11-28
医学信息(2016年29期)2016-11-28
中国现代医生(2016年23期)2016-11-15
中国实用医药(2016年24期)2016-10-17
上海医药(2016年17期)2016-10-12
科技视界(2015年30期)2015-10-22
中西医结合心血管病电子杂志(2014年14期)2015-07-25