体外循环下心脏手术患者围Me术ta期血糖严格控制与常规控制的 分析
2015-03-02 08:36曾庆东郭莎莎孙燕华李勇男吉冰洋
中国体外循环杂志 2015年2期
曾庆东,郭莎莎,孙燕华,刘 刚,周 琴,李勇男,吉冰洋,郑 哲
·临床研究·
体外循环下心脏手术患者围Me术ta期血糖严格控制与常规控制的 分析
曾庆东,郭莎莎,孙燕华,刘 刚,周 琴,李勇男,吉冰洋,郑 哲
目的 为了比较接受体外循环下心脏手术围术期血糖严格控制与常规控制患者的术后早期死亡率和相关并发症的发生率,利用现有的临床试验数据进行Meta分析。方法 计算机检索PubMed、EMBASE以及Cochrane library数据库,收集公开发表的有关对比体外循环下心脏手术围术期血糖严格控制与常规控制的文献,提取相关数据,并用RevMan 5.1进行数据分析。结果 共纳入14个随机对照试验,纳入人数总计2 732人。通过meta分析发现与常规血糖控制相比,严格血糖控制能降低术后早期死亡率(OR=0.62,95%CI[0.41,0.95],P=0.03)减少术后呼吸机辅助时间(SMD=-0.44,95%CI[-0.84,-0.04],P=0.03),但是增加了严重低血糖事件的发生率(OR=3.78,95%CI[1.58,9.02],P=0.003)。结论 与常规血糖控制相比,严格血糖控制能降低心脏手术患者术后早期死亡率并减少术后呼吸机辅助时间,但是增加了严重低血糖事件的发生率。
心脏手术;体外循环;血糖
体外循环辅助下心脏手术的围术期高血糖已经被证实为一个与术后早期死亡率及并发症相关的独立危险因素[1-2]。已有文献报道,无论对于糖尿病患者还是非糖尿病患者而言,接受心脏手术,特别是体外循环辅助下心脏手术时,围术期出现高血糖的风险都会明显增加[3-4]。因此,心脏手术围术期血糖控制问题越来越引起人们的关注。然而,近些年对于是否应该对接受体外循环辅助下心脏手术的患者进行严格的血糖控制存在着广泛的争议。本篇Meta分析旨在客观评价心脏手术围术期严格血糖控制所带来的收益与风险。
1 方法
本文采用Cochrane系统评价方法,对相关的文献进行质量评价和荟萃分析。纳入本篇Meta分析的文献必须符合以下标准:①随机对照试验(RCT);②试验的研究对象为接受体外循环辅助下心脏手术的成人患者;③试验组患者在术中和(或)术后接受严格血糖控制(血糖控制范围<8.3mmol/L);④对照组患者在术中和(或)术后接受常规血糖控制;⑤试验报道的结果中包含术后早期死亡率或者至少含有以下结果中的两种:围术期严重低血糖事件发生率、术后房颤、急性肾衰竭、神经系统并发症发生率、术后感染率、呼吸机辅助时间、术后ICU停留时间及术后住院日。
1.1 检索策略 根据流行病学指南,笔者系统性的检索了PubMed、Cochrane以及EMBASE,检索语言为英文,检索时间从数据库的创建一直到2014年10月,有两位作者分别进行检索最后进行对比,在做此次系统评价期间也会间断的检索这几个数据库,防止遗漏,同时还交叉检索了相关文献的参考文献。使用以下检索词进行自由组合:tight glycemic control、tight glucose control、strict glucose control、strict glycemic control、maintenance of glycaemia、management of hyperglycemia、perioperative glycemic control、intraoperative glucose control、perioperative insulin infusion、high-dose insulin treatment、intensive insulin therapy、cardiac surgery、extracorporeal circulation及cardiopulmonary bypass。未发表的以及会议摘要并未纳入研究。由两位作者单独进行文献检索以及数据的采集,最后进行结果比对,尽量避免遗漏和出错。
1.2 数据的提取 由两位作者使用统一的表格收集数据,并对纳入的文献使用JADA评分进行质量评价,两者的不同意见在本研究负责人的参与下通过协商解决。提取的数据包括作者、发表年代、样本量、JADA评分、分组情况、血糖控制范围、血糖控制时间以及试验结果等。见表1。
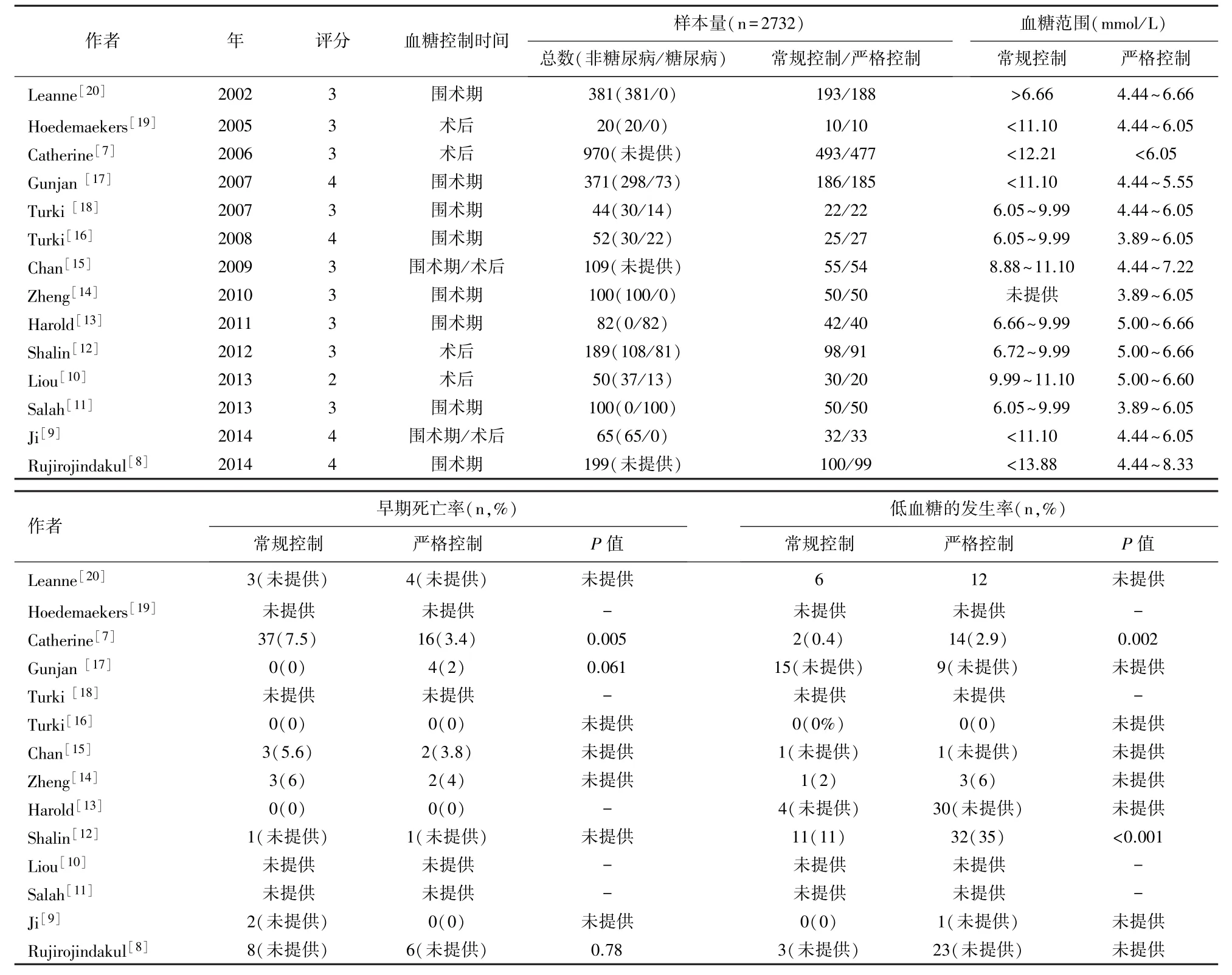
表1 纳入研究的基本特征
1.3 统计分析 对于二分类变量的数据,使用OR值来计算效应量;对于连续性变量,采用SMD来计算效应量。通过计算I2来评估统计学异质,I2<50%认为异质性较低,采用固定效应模型计算合并效应量;I2>50%则认为存在较大的异质性,使用随机效应模型对效应量进行合并。在一些研究中,提供呼吸机辅助时间和术后ICU停留时间及住院日为中位数值,笔者根据Cochrane Handbook将其转换为平均值。统计学软件采用RevMan 5.1,P≤0.05认为统计学差异显著。
2 结 果
2.1 文献检索流程及结果 按照以上检索策略,833条引文信息去重84条后剩余749篇潜在相关文献。通过阅读题目及摘要排除650篇无关文献后,对剩余的99篇文献通读全文,根据纳入标准排除了85篇文献(35篇综述,16篇研究对象并非接受心脏手术的成人患者,13篇与围术期血糖控制不相关,11篇信息数据不符合纳入标准,其中包含两篇将严格血糖控制组的血糖控制目标大于8.3 mmol/L的 RCT[5-6],以及10篇回顾性分析),最终,共纳入14个RCT,纳入人数总计2 732人[7-20]。
2.2 Meta分析结果
2.2.1 术后早期死亡率 共有8项研究报道了术后早期死亡率(n=2 384)[7-9,12,14-15,17,20]。 本研究将术后早期死亡率定义为术后30天内或在ICU内死亡的发生率。异质性检验:(P=0.46,I2=0),无显著异质性,故选用固定效应模型进行分析。与常规血糖控制组相比,严格血糖控制可以降低术后早期死亡率,且有统计学差异(OR=0.62,95%CI[0.41,0.95],P=0.03,Z=2.19)(图1)。
2.2.2 围术期严重低血糖发生率 共有9项研究报道了围术期低血糖发生率(n=2466)[7-9,12-15,17,20]。本研究将围术期严重低血糖定义为血糖值低于2.2 mmol/L。异质性检验:(P<0.0001,I2=76%)异质性较为显著,故选用随机效应模型进行分析。与常规血糖控制组相比,严格血糖控制增加了围术期严重低血糖发生率,且有统计学差异(OR=3.78,95%CI[1.58,9.02],P=0.003,Z=3.00)(图2)。
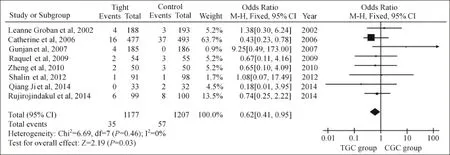
图1 两组术后早期死亡率的森林图(OR and 95%cofidence intervals)

图2 两组严重低血糖事件发生率的森林图(OR and 95%cofidence intervals)

图3 两组围术期并发症森林图(OR and 95%cofidence intervals)。
2.2.3 术后感染率,围术期及术后房颤、神经系统并发症、急性肾衰竭发生率 与常规血糖控制组相比,严格血糖控制可以降低术后感染率(OR=0.79,95%CI[0.52,1.18],P=0.25,Z=1.16),围术期房颤发生率(OR=0.87,95%CI[0.64,1.18],P=0.36,Z=0.91),神经系统并发症发生率(OR=0.69,95%CI[0.16,2.98],P=0.60,Z=0.52),但两组间无明显的统计学差异。在急性肾衰竭发生率方面,两组结果相似(图3)。
2.2.4 呼吸机辅助时间、术后ICU停留时间及住院日 在呼吸机辅助时间组,异质性检验:(P<0.00001,I2=87%)异质性较为显著,故选用随机效应模型进行分析。与常规血糖控制组相比,严格血糖控制可以减少呼吸机辅助时间,且有统计学差异(SMD=-0.44,95%CI=[-0.84,-0.04],P=0.03,Z=2.14)。在术后ICU停留时间及住院日方面,两组结果相似(图4)。
3 讨 论
本篇Meta分析结果显示,对于接受体外循环辅助下心脏手术的成人患者而言,与常规的血糖控制相比,严格的血糖控制可以降低术后早期死亡率,减少呼吸机辅助时间,同时增加了围术期严重低血糖的风险,并具有统计学差异。
非缺血状态下心肌的能量供应主要来源于游离脂肪酸的氧化磷酸化[21]。体外循环过程中,心肌处于缺氧状态,游离脂肪酸无法正常代谢,蓄积的游离脂肪酸抑制了葡萄糖的氧化并刺激了葡萄糖在肝脏的合成,使血糖水平升高[22]。外科手术及体外循环促进了包括胰高血糖素、皮质醇及儿茶酚胺类激素的释放,造成了外周胰岛素抵抗。同时,胰岛素与体外循环管道的直接接触,进一步破坏了胰岛素的功能[2,23]。此外,术中及术后大量的肝素及儿茶酚胺类药物的应用也会影响糖代谢,使血糖浓度升高[24-25]。
高血糖会促进炎症反应,同时影响血管内皮功能,从而降低了一氧化氮活性,并增加了超氧自由基的产生[26-29]。此外,炎症反应会导致血管的氧化应激,促进血管内血栓形成、斑块破裂并影响血小板功能[30]。另外,高血糖还会影响单核细胞、中性粒细胞及内皮细胞功能,进而增加术后感染的风险[31]。
本Meta分析结果显示,严格血糖控制可以降低术后早期死亡率,这一结果与Van den Berghe等于2001年发表的结果一致[32],而与Finfer等(NICESUGAR研究)2009年发表的结果相反[33]。主要原因可能是研究对象不同:Van den Berghe的研究中,研究对象为外科手术后的ICU患者,且其中67%的患者接受的是心脏手术;而Finfer的研究中,研究对象为混合的ICU患者,其中手术后患者比例仅为37%;而纳入本Meta分析的研究对象均为接受体外循环辅助下心脏手术的患者。一篇纳入了26个随机对照研究的Meta分析已经报道严格的血糖控制仅对外科ICU患者有益,而对内科或混合ICU并无益处[34]。
本Meta分析结果显示,严格血糖控制增加了围术期严重低血糖事件的发生风险,这与Finfer发表的结果一致[33]。严重的低血糖对于患者来说同样是危险的,它既可以增加早期死亡率,同时也会增加术后并发症,特别是神经系统并发症[35]。因此,如果能够在进行严格血糖控制的同时避免或者减少严重低血糖事件的发生,那么将会进一步增加严格血糖控制的收益。为了避免严重低血糖事件的发生,需要做到以下几个方面:①制定科学合理的血糖控制及营养支持方案;②及时并且精确地检测血糖浓度;③组建由外科医生、麻醉医生、体外循环医生、ICU医生、护士共同组成的团队以保证血糖控制的安全性和有效性。已经有研究报道,运用科学合理的血糖控制方案,可以成功的将严格血糖控制组的严重低血糖事件发生率控制在1%以下[17,36]。

图4 两组术后呼吸机辅助时间森林图(SMD and 95%cofidence intervals)
严格血糖控制与患者预后的关系,对于糖尿病患者和非糖尿病患者而言可能是不同的。相比于非糖尿病患者,糖尿病患者对于高血糖期间血糖波动的耐受性更好[37]。一篇回顾性分析报道,血糖水平为8~10mmol/L和10~11mmol/L的非糖尿病患者的术后早期死亡率分别为相同血糖水平的糖尿病患者的1.7倍和3.3倍[38]。纳入本研究的14个RCT中,有 2个 RCT的研究对象全部为糖尿病患者[11,13],4个RCT的研究对象全部为非糖尿病患者[9,14,19-20]。笔者对非糖尿病患者组术后早期死亡率进行了亚组分析,结果没有明显的统计学差异(OR=0.76,95%CI[0.27,2.15],P=0.61),这可能与样本量太小有关。因此,目前迫切需要一个区别对待糖尿病患者与非糖尿病患者大规模的多中心临床试验来给出结论。
本研究存在一定的局限性,主要有一下几方面:①纳入的研究中,试验组与对照组的血糖控制标准不一致;②开始进行严格血糖控制的时间点及持续的时间段不一致;③各个被纳入的研究,其研究对象中糖尿病患者与非糖尿病患者比例不一致(表1)。
总之,与常规血糖控制相比,严格血糖控制能降低心脏手术患者术后早期死亡率并减少术后呼吸机辅助时间,但是增加了严重低血糖事件的发生率。由于本篇meta分析存在一定的局限性,这一结论仍需大规模多中心临床RCT的验证。
[1] Knapik P,Nadziakiewicz P,Urbanska E,et al.Cardiopulmonary bypass increases postoperative glycemia and insulin consumption after coronary surgery[J].Ann Thorac Surg,2009,87(6):1859-1865.
[2] Giakoumidakis K,Nenekidis I,Brokalaki H.The correlation between peri-operative hyperglycemia and mortality in cardiac surgery patients:a systematic review[J].Eur JCardiovasc Nurs,2012,11(1):105-113.
[3] Gandhi GY,Nuttall GA,Abel MD,et al.Intraoperative hyperglycemia and perioperative outcomes in cardiac surgery patients[J].Mayo Clin Proc,2005,80(7):862-866.
[4] Doenst T,Wijeysundera D,Karkouti K,et al.Hyperglycemia during cardiopulmonary bypass is an independent risk factor for mortality in patients undergoing cardiac surgery[J].J Thorac Cardiovasc Surg,2005,130(4):1144.
[5] Giakoumidakis K,Eltheni R,Patelarou E,et al.Effects of intensive glycemic control on outcomes of cardiac surgery[J].Heart Lung,2013,42(2):146-151.
[6] Lazar HL,Chipkin SR,Fitzgerald CA,etal.Tightglycemic control in diabetic coronary artery bypass graft patients improves perioperative outcomes and decreases recurrent ischemic events[J].Circulation,2004,109(12):1497-1502.
[7] Ingels C,Debaveye Y,Milants I,etal.Strict blood glucose control with insulin during intensive care after cardiac surgery:Impact on 4-years survival,dependency onmedical care,and quality-of-life[J].Eur Heart J,2006,27(22):2716-2724.
[8] Rujirojindakul P,Liabsuetrakul T,McNeil E,et al.Safety and efficacy of intensive intraoperative glycaemic control in cardiopulmonary bypass surgery:a randomised trial[J].Acta Anaesthesiol Scand,2014,58(5):588-596.
[9] Ji Q,DingW,Mei Y,et al.Protective Effects of Tight Glucose Control During Cardiopulmonary Bypass on Myocardium in Adult Nondiabetic Patients Undergoing Valve Replacement[J].Can J Cardiol,2014,30(1):1429-1435.
[10] Liou HL,Shih CC,Chung KC,etal.Comparison of the effectof intensive versus conventional insulinotherapy in patients with cardiac surgery after cardiopulmonary bypass[J].Chin J Physiol,2013,56(2):101-109.
[11] Asida SM,Atalla MMM,Gad GS,et al.Effect of perioperative control of blood glucose level on patient's outcome after anesthesia for cardiac surgery[J].Egyptian Journal of Anaesthesia,2013,29:71-76.
[12] Desai SP,Henry LL,Holmes SD,et al.Strict versus liberal target range for perioperative glucose in patients undergoing coronary artery bypass grafting:a prospective randomized controlled trial[J].JThorac Cardiovasc Surg,2012,143(2):318-325.
[13] Lazar HL,McDonnell MM,Chipkin S,et al.Effects of aggressive versusmoderate glycemic control on clinical outcomes in diabetic coronary artery bypass graft patients[J].Ann Surg,2011,254(3):458-463.
[14] Zheng R,Gu C,Wang Y,et al.Impacts of intensive insulin therapy in patients undergoing heart valve replacement[J].Heart Surgery Forum,2010,13(5):E292-E298.
[15] Chan RP,Galas FR,Hajjar LA,et al.Intensive perioperative glucose control does not improve outcomes of patients submitted to open-heart surgery:a randomized controlled trial[J].Clinics(Sao Paulo),2009,64(1):51-60.
[16] Albacker T,Carvalho G,Schricker T,et al.High-dose insulin therapy attenuates systemic inflammatory response in coronary artery bypass grafting patients[J].Ann Thorac surg,2008,86(1):20-27.
[17] Gandhi GY,Nuttall GA,Abel MD,et al.Intensive intraoperative insulin therapy versus conventional glucosemanagement during cardiac surgery:A randomized trial[J].Ann Intern Med,2007,146(4):233-243.
[18] Albacker TB,Carvalho G,Schricker T,etal.Myocardial protection during elective coronary artery bypass grafting using highdose insulin therapy[J].Ann Thorac Surg,2007,84(6):1920-1927.
[19] Hoedemaekers CW,Pickkers P,Netea MG,et al.Intensive insulin therapy doesnotalter the inflammatory response in patientsundergoing coronary artery bypass grafting:a randomized controlled trial[J].Crit care,2005,9(6):790-797.[20] Groban L,Butterworth J,Legault C,et al.Intraoperative insulin therapy does not reduce the need for inotropic or antiarrhythmic therapy after cardiopulmonary bypass[J].J Cardiothorac Vasc Anesth,2002,16(4):405-412.
[21] Opie LH.Effects of regional ischemia on metabolism of glucose and fatty acids.Relative rates of aerobic and anaerobic energy production during myocardial infarction and comparison with effects of anoxia[J].Circ Res,1976,38(5 Suppl 1):I52-74.
[22] Lazzeri C,Bevilacqua S,Ciappi F,et al.Glucosemetabolism in cardiovascular surgery[J].HSR Proc Intensive Care Cardiovasc Anesth,2010,2(1):19-26.
[23] O'Connor CJ.Glycemic control during cardiac surgery:a moving target[J]?Curr Opin Anaesthesiol,2010,23(1):47-48.
[24] Bulow NM,Barbosa NV,Rocha JB.Opioid consumption in total intravenous anesthesia is reduced with dexmedetomidine:a comparative study with remifentanil in gynecologic videolaparoscopic surgery[J].JClin Anesth,2007,19(4):280-285.
[25] Malmström R,Packard CJ,Caslake M,et al.Effectof heparinstimulated plasma lipolytic activity on VLDL APO B subclassmetabolism in normal subjects[J].Atherosclerosis,1999,146(2):381-390.
[26] Dandona P,Aljada A,Mohanty P,et al.Insulin inhibits intranuclear nuclear factor kappaB and stimulates IkappaB inmononuclear cells in obese subjects:evidence for an anti-inflammatory effect[J]?JClin EndocrinolMetab,2001,86(7):3257-3265.
[27] Guerci B,Böhme P,Kearney-Schwartz A,et al.Endothelial dysfunction and type 2 diabetes.Part 2:altered endothelial function and the effects of treatments in type 2 diabetesmellitus[J].Diabetes Metab,2001,27(4 Pl 1):436-447.
[28] Park JY,Takahara N,Gabriele A,et al.Induction of endothelin-1 expression by glucose:an effect of protein kinase C activation[J].Diabetes,2000,49(7):1239-1248.
[29] Guzik TJ,Mussa S,Gastaldi D,et al.Mechanisms of increased vascular superoxide production in human diabetesmellitus:role of NAD(P)H oxidase and endothelial nitric oxide synthase[J].Circulation,2002,105(14):1656-1662.
[30] Marfella R,Esposito K,Giunta R,et al.Circulating adhesion molecules in humans:role of hyperglycemia and hyperinsulinemia[J].Circulation,2000,101(19):2247-2251.
[31] Perner A,Nielsen SE,Rask-Madsen J.High glucose impairs superoxide production from isolated blood neutrophils[J].Intensive Care Med,2003,29(4):642-645.
[32] Van den Berghe G,Wouters P,Weekers F,etal.Intensive insulin therapy in critically ill patients[J].N Engl JMed,2001,345(19):1359-1367.
[33] NICE-SUGAR Study Investigators,Finfer S,Chittock DR,etal.Intensive versus conventional glucose control in critically ill patients[J].N Engl JMed,2009,360(13):1283-1297.
[34] Griesdale DE,de Souza RJ,van Dam RM,etal.Intensive insulin therapy and mortality among critically ill patients:ameta-analysis including NICE-SUGAR study data[J].CMAJ,2009,180(8):821-827.
[35] Abdelmalak BB,Lansang MC.Revisiting tightglycemic control in perioperative and critically ill patients:when one sizemay not fit all[J].JClin Anesth,2013,25(6):499-507.
[36] Lecomte P,Foubert L,Nobels F,et al.Dynamic tight glycemic control during and after cardiac surgery is effective,feasible,and safe[J].Anesth Analg,2008,107(1):51-58.
[37] American Diabetes Association.Standards ofmedical care in diabetes--2009[J].Diabetes Care,2009,Suppl 1:S13-61.
[38] Egi M,Bellomo R,Stachowski E,et al.Blood glucose concentration and outcome of critical illness:the impactof diabetes[J].Crit Care Med,2008,36(8):2249-2255.
Tight glycem ic control versus conventional glycem ic control during cardiac surgery w ith cardiopulmonary bypass:a M eta-Analysis
Zeng Qing-dong,Guo Sha-sha,Sun Yan-hua,Liu Gang,Li Yong-nan,Zhou Qin,Ji Bing-yang,Zheng Zhe Department ofCardiopulmonary Bypass,Fuwai Hospital,National center for Cardiovascular disease,Chinese Academy ofMedical science and Peking Union Medical College,Beijing,100037,China Corresponding author:Ji Bingyang,E-mail:jibingyang@fuwai.com
ObjectiveThe aim of thismeta-analysis is to determine the effect of tight versus conventional glycemic control during cardiac surgery with cardiopulmonary bypass(CPB)on measures ofmorbidity and mortality.MethodsStudies in which adult cardiac surgical patientswere assigned randomly to tight glycemic control(TGC)versus conventional glycemic control(CGC)were searched through PubMed,EMBASE,and the Cochrane Central Register of Controlled Trials.Data extracted from identified studies were analyzed using RevMan 5.1.The resultswere presented as odd ratio(OR)and standardized mean difference(SMD)with 95% confidence intervals(CIs).ResultsFourteen randomized controlled trials that included 2732 patientswere identified,although notall trials could be used in each analysis.Tight glycemic control reduced earlymortality after surgery(OR=0.62,95%CI[0.41,0.95],P=0.03)and themechanical ventilation time(SMD=-0.44,95%CI[-0.84,-0.04],P=0.03),while it conversely increased the incidence ofhypoglycemia(OR=3.78,95%CI[1.58,9.02],P=0.003).ConclusionIntraoperative use of TGCmay decrease earlymortality and shorten themechanical ventilation time in patients undergoing cardiac surgery with CPB,conversely increase the incidence of hypoglycemia compared with CGC group.Beneficial effects of TGCmay be demonstrated when the appropriate glycemic targets arematched to the appropriate population.
Cardiac surgery;Cardiopulmonary bypass;Glycemic
2015-04-07)
2015-04-15)
10.13498/j.cnki.chin.j.ecc.2015.02.02
100037北京,北京协和医学院中国医学科学院国家心血管病中心阜外医院体外循环科(曾庆东、郭莎莎、孙燕华、刘 刚、周 琴、李勇男、吉冰洋),心脏外科(郑 哲)
通迅作者:吉冰洋,E-mail:jibingyang@fuwai.com
猜你喜欢
中国现代医生(2022年21期)2022-08-22
中国典型病例大全(2022年11期)2022-05-13
锦州医科大学报(2022年2期)2022-05-07
保健与生活(2022年9期)2022-05-06
——体外循环质量控制的基石
中国体外循环杂志(2021年2期)2021-11-30
中华养生保健(2020年7期)2020-11-16
医学新知(2019年4期)2020-01-02
中国体外循环杂志(2019年4期)2019-09-13
饮食保健(2019年2期)2019-01-17
妇女之友(2016年11期)2017-01-20