
Anti-IgLON5 disease: a novel topic beyond neuroimmunology
2022-09-27 09:44YiZongHengZhangYouNiYiNingGaoDingDingShenLuHeDouYinHuanYuMengQinMingZhouJiHuShengChen
中国神经再生研究(英文版) 2023年5期
Yi-ZongHeng Zhang , You Ni , Yi-Ning Gao , Ding-Ding Shen , Lu He Dou Yin Huan-Yu Meng Qin-Ming Zhou ,Ji Hu, , Sheng Chen ,
Abstract Anti-IgLON5 disease is a recently defined autoimmune disorder of the nervous system associated with autoantibodies against IgLON5.Given its broad clinical spectrum and extremely complex pathogenesis,as well as difficulties in its early diagnosis and treatment, anti-IgLON5 disease has become the subject of considerable research attention in the field of neuroimmunology.Anti-IgLON5 disease has characteristics of both autoimmunity and neurodegeneration due to the unique activity of the anti-IgLON5 antibody.Neuropathologic examination revealed the presence of a tauopathy preferentially affecting the hypothalamus and brainstem tegmentum, potentially broadening our understanding of tauopathies.In contrast to that seen with other autoimmune encephalitis-related antibodies, basic studies have demonstrated that IgLON5 antibody-induced neuronal damage and degeneration are irreversible, indicative of a potential link between autoimmunity and neurodegeneration in anti-IgLON5 disease.Herein, we comprehensively review and discuss basic and clinical studies relating to anti-IgLON5 disease to better understand this complicated disorder.
Key Words: anti-IgLON5 disease; autoimmune encephalitis; human leukocyte antigen; IgG4-related diseases; IgLON5 antibody; IgLONs; immunotherapy; inflammation; neurodegeneration;neuroimmunology; tauopathy
Introduction
Anti-IgLON5 disease is a rare autoimmune neurological disorder associated with autoantibodies against the IgLON5 protein.In 2014, Sabater et al.reported six patients presenting with IgLON5 antibodies, unique rapid eye movement and non-rapid eye movement sleep disorders, and tau deposition.A growing number of cases have since been reported and have revealed the heterogeneity of the disease.Most patients experience chronic onset and no gender differences have been identified (Grüter et al., 2022).Patients may present with sleep disorders, bulbar syndrome, gait instability, cognitive impairment, and movement disorders (Sabater et al., 2014).The human leukocyte antigen (HLA)-DRB1*10:01-DQB1*05:01 haplotype is strongly associated with the disease, indicating that genetic factors may contribute to anti-IgLON5 disease susceptibility (Gaig et al., 2019).
Tau deposits mainly involving the hypothalamus and brainstem tegmentum have been found in several patients (Sabater et al., 2014; Gelpi et al., 2016),hinting at a correlation between autoimmunity and neurodegeneration in this disease.Basic studies have investigated the long-term effects of the anti-IgLON5 antibody, which may include inflammation and neuronal damage(Sabater et al., 2016; Ni et al., 2022a).Disruption of the blood-brain barrier and intrathecal lymphocytosis have also been identified, confirming the importance of autoimmunity (Strippel et al., 2022).Additionally, the anti-IgLON5 antibody seems to play a central role in this disease, implying that neurodegeneration in anti-IgLON5 disease may be a consequence of autoimmunity.
Reviews focusing on anti-IgLON5 disease are scarce and mostly concerned with clinical manifestations.Herein, we review published clinical and basic research on anti-IgLON5 disease, mainly focusing on newly discovered features, including clinical and imaging features, diagnostic clues, and treatment prognosis.We also analyze the unique tauopathy and experiments relating to anti-IgLON5 disease aiming to understand its pathogenesis and discuss the challenges and directions for future study.
Literature Search Strategy
In this review, PubMed was searched for articles published until June 2022.The following keywords were used for the literature search: IgLON5, anti-IgLON5 disease, IgLON5 antibody, IgLON, IgG4-related diseases, tauopathy,neurodegeneration, and inflammation.Only publications in English were screened.
The Structure and Function of IgLON5
IgLON5 is a cell adhesion molecule belonging to the IgLON family.Members of this family are characterized by an N-terminal signal peptide, three Iglike domains, and a glycosylphosphatidylinositol (GPI) anchor (Vanaveski et al., 2017).The IgLON family comprises five members, namely, opioid binding protein/cell adhesion molecule (OPCML), neurotrimin (NTM), limbic system associated membrane protein (LSAMP), neural growth regulator 1 (NEGR1),and IgLON family member 5 (IgLON5).IgLONs form homo- or heterodimers both in cis (on the same membrane) and in trans (between cells) (Reed et al., 2004; Vanaveski et al., 2017; Venkannagari et al., 2020).Ranaivoson et al.(2019) and Venkananagari et al.(2020) analyzed the crystal structure of IgLONs and identified several possible configurations (Figure 1).IgLONs participate in neural development and neural circuit formation (Karis et al.,2018), and may also be involved in tumor inhibition, depression, and obesity(Karis et al., 2018).
In humans, IgLON5 proteins are mainly expressed in the brain and testis.In the brain, the highest IgLON5 protein levels are found in the cerebellum.Meanwhile, IgLON5 transcripts are distributed in a wide variety of tissues, but particularly in the brain, retina, and testis (https://www.proteinatlas.org/).However, the distribution of IgLON5 transcripts in mice differs from that in humans (Vanaveski et al., 2017), with mice displaying the highest IgLON5 RNA expression in the thalamus and pons.IgLON5 transcripts are also abundantly present in mouse skeletal muscle but are absent in the liver (Vanaveski et al.,2017).
The function of IgLON5 remains mostly obscure.Lim et al.(2021)demonstrated that IgLON5 regulates the adhesion and differentiation of myoblasts and promotes myogenesis and regeneration.Interestingly,the authors reported that the antibody-mediated inhibition of IgLON5 in myoblasts led to a compensatory increase in IgLON5 mRNA and protein expression levels.Additionally, IgLON5 transcript levels were found to be markedly lower in the dorsolateral prefrontal cortex of schizophrenic patients who committed suicide than in those who did not, suggestive of a potential role for IgLON5 in central nervous systems development and regulation(Karis et al., 2018).IgLON5 levels may also be negatively correlated with the prognosis of colon cancer (Chen et al., 2021) and positively associated with limonin-mediated cardiac repair after myocardial infarction (Xiong et al.,2021).More studies on the role of anti-IgLON5 disease are needed to reveal the functions of IgLON5, the last member of the IgLON family to be identified.
Current Knowledge of Anti-IgLON5 Disease:Clinical Features, Diagnosis, and Treatment
Clinical features and imaging characteristics
Several cases of anti-IgLON5 disease have been reported since its discovery and they display significant heterogeneity.Relevant clinical studies performed from 2014 to 2022 are summarized in Additional Table 1.Previous reviews have fully described the core clinical phenotypes, which include sleep disorders, bulbar syndrome, gait instability, and cognitive impairment(Madetko et al., 2022).Dysautonomia, oculomotor abnormalities, and neuropsychiatric symptoms are also frequently reported (Grüter et al., 2022),as are movement disorders, with 87% (63/72) of patients having at least one type of dyskinesia (Gaig et al., 2021).
The range of symptoms has gradually expanded as more patients are identified.One patient with tau deposition, mainly in the cerebellum,displayed obvious symptoms associated with cerebellar dysfunction, such as intention tremors and nystagmus (Schöberl et al., 2018).Peripheral neuropathy has also been observed in several patients (Honorat et al., 2017;Hansen et al., 2020; Macher et al., 2021), implying that the effects of anti-IgLON5 antibodies may extend to the peripheral nervous system.Some patients had paresthesia, which manifested as tongue neuralgia (Haitao et al., 2016), peripheral facial paralysis (Schröder et al., 2016), and cold intolerance (Morales-Briceño et al., 2018; Aslam and Shill, 2020).Some cases may present as motor neuron disease.For instance, Tao et al.(2018)described a patient who displayed progressive dysphagia and limb weakness with muscle atrophy.Electromyography showed extensive denervation in limb and thoracic paraspinal muscles.Epilepsy has also been observed in patients with anti-IgLON5 disease, although only rarely.One case series identified electrographic seizures without clinical manifestation in one patient (Honorat et al., 2017); however, only a few cases of epilepsy have been described since then (Macher et al., 2018, 2021; Montagna et al., 2018; Chen et al., 2020;Stoyanov et al., 2021; Fu et al., 2022; Ni et al., 2022b; Wang et al., 2022).Recently, Fu et al.(2022) found signs of inflammation in the hippocampus of a patient who experienced seizures as the main symptom, suggesting inflammation-induced hyperexcitability.Ni et al.(2022b) identified some unusual manifestations, such as “dancing belly and restless legs syndrome”.Takotsubo cardiomyopathy, a fatal condition, was observed in one patient during stridor (Montojo et al., 2016).Another case reported the occurrence of pop music hallucinations, which had never been observed before (Stoyanov et al., 2021).
New cases can provide novel insights into the occurrence and development of the disease.A few patients demonstrated influenza-like illnesses and exhibited headache, fever, and vomiting (Chen et al., 2020; Swayne et al.,2021; Wang et al., 2021).Both the Epstein-Barr virus (Ni et al., 2022b) and the herpes virus (Wang et al., 2022) have been reported in patients with anti-IgLON5 disease.A few patients also had other autoimmune diseases, such as vitiligo, Hashimoto’s thyroiditis, and connective tissue disease (Haitao et al.,2017; Honorat et al., 2017; Ni et al., 2022b; Grüter et al., 2022).Notably, a 2-year-old boy with Langerhans cell histiocytosis showed IgLON5 antibodies in serum (Ye et al., 2021).He was the youngest patient reported.Furthermore,the IgLON5 antibody was found to coexist with other antibodies, such as LGI1 (Honorat et al., 2017; Ni et al., 2022b), GAD65 (Honorat et al., 2017),gamma-aminobutyric acid type B receptor (Chung et al., 2019), amphiphysin(Grüter et al., 2022), and MOG (Ni et al., 2022b), indicative of B-lymphocyte dysfunction.The role of these coexisting antibodies in anti-IgLON5 disease pathogenesis requires further study.Importantly, diagnosis should be carefully managed because it is difficult to determine the primary ‘culprit’ antibody.
Gaig et al.(2021) documented that 76% (55/76) of patients with anti-IgLON5 disease had some form of chronic manifestation (> 4 months) while another clinical study reported that approximately 28% (15/53) of patients had acute to subacute manifestations (≤ 4 weeks) (Grüter et al., 2022).Subacute manifestations are associated with inflammation-related changes in the cerebrospinal fluid (CSF) and are regarded as part of the early period of the disease (Grüter et al., 2022).Pathologies previously described by Gelpi et al.(2016) included a lack of inflammation and the presence of p-tau deposition mainly in the hypothalamus and brainstem tegmentum; however, subsequent cases did not involve tauopathy (Montagna et al., 2018; Morales-Briceño et al., 2018).The differences in clinical features and pathological changes highlight the heterogeneous nature of this disorder.
Patients with anti-IgLON5 disease can display diverse magnetic resonance imaging (MRI) changes.In one study, 12.5% (9/72) patients had distinct alterations on MRI (Tagliapietra et al., 2021).Brain atrophy (Gaig et al., 2017;Honorat et al., 2017; Macher et al., 2021), T2 hyperintensity (Macher et al.,2018; Ramanan et al., 2018; Wang et al., 2022), and white matter changes(Honorat et al., 2017; Macher et al., 2021; Ni et al., 2022b; Videnovic et al.,2022) have all been observed, in addition to other signs (Additional Table 1)mainly involving the hippocampus, brainstem, white matter, cerebellum, and cortex.Recently, “high-convexity tight sulci” (defined as the compression of sulci at the vertex, enlarged CSF spaces in the Sylvian fissure, and ventriculomegaly)on MRI, a marker of CSF dynamics problems, was reported in one patient(Urso et al., 2022).Hyperperfusion was also seen in the high-convexity area on single-photon emission computed tomography and arterial spin labeling-MRI,which may reflect the increased gray matter density of the convexity (Urso et al., 2022).Additionally, single-photon emission computed tomography imaging using dopamine transporter radioligands showed decreased ligand uptake mostly in the striatum (Montojo et al., 2016; Fuseya et al., 2020; González-Ávila et al., 2021), suggesting that the dopaminergic pathway had had been affected (González-Ávila et al., 2021).Meanwhile, onF-FDG positron emission tomography scans, some patients displayed hypermetabolism in the basal ganglia (Haitao et al., 2016, 2017; Zhang et al., 2016; Morales-Briceño et al.,2018; Ni et al., 2022b), cerebellum (Haitao et al., 2016; Zhang et al., 2016),brainstem (Morales-Briceño et al., 2018), and other areas (Haitao et al., 2017;Wang et al., 2022).White matter and left temporal lobe hypometabolism has also been observed in some patients (Ni et al., 2022b).
Diagnosis
At present, anti-IgLON5 disease diagnosis is mainly based on clinical manifestations and the detection of IgLON5 antibodies in serum and/or CSF of patients.The most common symptoms at diagnosis are sleep disorders,bulbar syndrome, movement disorders, cognitive impairment, oculomotor abnormalities, and dysautonomia.Most patients have IgLON5 antibodies in both serum and CSF, which can help confirm diagnosis (Grüter et al., 2022).The serum antibody titer increases with disease duration and decreases after long-term immunotherapy.IgG4 is the most commonly identified subtype,followed by IgG1 and IgG2 (Gaig et al., 2017; Grüter et al., 2022).
Other tests may be helpful for diagnosis.Recently, signs of inflammation in the CSF or on MRI have been reported in some patients (Montagna et al.,2018; Hansen et al., 2020; Grüter et al., 2022; Strippel et al., 2022), and may be a predictor of the initial stage of anti-IgLON5 disease.Meanwhile, HLA genotyping may represent a means of identifying susceptible patients.The HLA-DRB1*10:01 and HLA-DQB1*05:01 alleles are highly present in patients with anti-IgLON5 disease (Sabater et al., 2014), with HLA-DRB1*10:01 confirmed as having a stronger correlation with the disease than HLADQB1*05:01 (Gaig et al., 2017).Employing prediction algorithms, Gaig et al.(2019) determined a strong binding affinity between the IgLON5 peptide and HLA-DRB1 molecules.They also found that patients carrying HLA-DRB1*10:01 were more prone to sleep abnormalities, medulla oblongata dysfunction,and autonomic dysfunction; however, cognitive impairment was associated with being HLA-DRB1*10:01-negative.In contrast, Grüter et al.(2022)did not report finding the same associations, except for the link between sleep disorders and the HLA-DRB1*10:01 and HLA-DQB1*05:01 alleles.Notably, they also observed younger ages in both HLA-DRB1*10:01 and HLADQB1*05:01 carriers than HLA-DRB1*non-10:01 and HLA-DQB1*non-05:01 carriers, and anti-IgLON5 IgG titers were higher in patients with HLADRB1*10:01 than in those with HLA-DRB1*non-10:01.This evidence links genotype and phenotype, providing guidance for the diagnosis and treatment of anti-IgLON5 disease.
Regarding pathology, the detection of hyperphosphorylated tau protein can serve as important evidence in anti-IgLON5 disease diagnosis.Gelpi et al.(2016) proposed the establishment of levels of certainty-definite, probable,and possible—as criteria for the diagnosis of anti-IgLON5-related tauopathy.The levels of certainty are mainly based on pathology, autoantibody, HLA genotype/clinical history.Although these criteria are helpful for diagnosis,they have limitations.Evidence from both clinical and basic studies has shown that tau deposition occurs in the late stages of anti-IgLON5 disease;however, not all patients can be diagnosed at this stage, which may result in pathological changes going undetected.
The mortality rate is higher for anti-IgLON5 disease than for other types of autoimmune encephalitis (AE) (Sabater et al., 2014), particularly in patients with respiratory disorders.It can be inferred from existing cases that laryngeal spasm (Tagliapietra et al., 2021), respiratory failure (Honorat et al., 2017),central hypoventilation (Grüter et al., 2022), aspiration pneumonia (Högl et al., 2015), and cardiac complications (Cagnin et al., 2017; Gaig et al., 2017;Grüter et al., 2022) are the most likely causes of death.Extra care must be taken when treating patients with these symptoms.
Treatment progress
The prognosis for patients with anti-IgLON5 disease, even with treatment, is assumed to be poor (Sabater et al., 2014; Gaig et al., 2017).Nevertheless,recent studies have suggested that patients may benefit from immunotherapy,although whether immunotherapy can improve the long-term prognosis of the disease remains unknown (Grüter et al., 2022).The main treatment consists of first- and second-line immunotherapy as well as symptomatic therapies.First-line therapy is the treatment of choice and comprises steroids,intravenous immunoglobulin, and plasmapheresis (Tagliapietra et al., 2021).The response rate to first-line therapy was reported to be 55.8% (39/70),while that to second-line therapy, such as rituximab, cyclophosphamide,azathioprine, and mycophenolate mofetil, was 63% (17/27) (Fu et al., 2022).
Moreover, one study revealed that 52.9% (27/51) patients had relapse-like exacerbations during the course of the disease (Grüter et al., 2022).Among these, 41% (11/27) showed improvement after first-line therapy.In the same study, long-term immunotherapy, including first- and second-line therapy,was found to be effective in 75% (27/36) patients.In general, immunotherapy seems to be more effective than was previously thought and can be effective in half of the patients.Long-term use may benefit an even greater number of patients.
Factors other than drug selection may also affect prognosis.Patients who develop anti-IgLON5 disease and already have a chronic disease were reported to be more likely to relapse or deteriorate due to late discovery,while those with acute and subacute attacks were typically diagnosed earlier (Grüter et al., 2022).Patients with cognitive impairment and atypical phenotypes showed better outcomes than those with typical symptoms such as sleep and bulbar disorders (Cabezudo-García et al., 2020).Early treatment is crucial for patients (Grüter et al., 2020; Pi et al., 2021).Grüter et al.(2022)identified that the initiation of short-term, first-line treatment within 6 weeks of initial deterioration, or the initiation of long-term treatment within 1 year of onset, were predictors of clinical improvement; moreover, a low serum level of neurofilament light chain before treatment was found to be correlated with a better prognosis.
The presence of inflammation may be indicative of early-stage disease and its identification is likely to be associated with better outcomes (Montagna et al.,2018; Cabezudo-García et al., 2020; Hansen et al., 2020).Grüter et al.(2022)reported that 37.3% (19/51) patients exhibited inflammation-related changes in the CSF, while the CSF cell count was negatively correlated with disease duration.Approximately 8.1% (4/49) of patients had IgLON5 antibodies only in serum (Tagliapietra et al., 2021) and some of these patients recovered after immunotherapy (Pi et al., 2021; Wang et al., 2021).Several studies reported poor outcomes in patients with IgG4 subtype predominance (Högl et al.,2015; Simabukuro et al., 2015; Haitao et al., 2017; Ni et al., 2022b).However,this effect seemed to be associated with HLA-DRB1*10:01 negativity, which is related to better outcomes (Gaig et al., 2019; Werner et al., 2021).Additional studies are needed to clarify the relationship between antibody subtypes,genotypes, and prognosis.
A recent study revealed an increase in B cell numbers and the presence of plasma cells in the CSF of patients with IgLON5 disease.Patients with plasma cells in the CSF responded well to rituximab (Strippel et al., 2022).This observation explains the key role of B cells and antibodies in the pathogenesis of the disease and confirms the effectiveness of anti-B cell drugs.In addition,anti-B cell drugs, such as rituximab, have been confirmed to be effective in treating IgG4-related diseases (Dalakas, 2021, 2022) and, thus, may be a better choice for treatment.Additional strategies may be developed once the underlying mechanisms have been determined.
Research Progress on the Pathogenicity of the IgLON5 Antibody
Auto-IgLON5 antibody-related tauopathy: Broadening our understanding of tauopathies
Anti-IgLON5 disease has been associated with tau deposition since its discovery.Sabater et al.(2014) were the first to report tau deposition in patients with anti-IgLON5 disease in 2014.Neuropathological examination revealed p-tau deposition mainly in the hypothalamus and brainstem tegmentum.Gelpi et al.(2016) proposed the concept of anti-IgLON5 diseaserelated tauopathy and summarized its possible pathological features, including neuronal loss, gliosis, and lack of inflammatory infiltration.Consistent with the pathological analysis, a few patients had increased tau and p-tau levels in the CSF (Brüggemann et al., 2016; Vetter et al., 2018; Logmin et al., 2019;Grüter et al., 2022; Hansen et al., 2020).
However, some patients do not exhibit the above typical pathology.One patient showed tau deposition mainly involving the cerebellum (Schöberl et al., 2018).Notably, this patient had inflammation in the leptomeningeal area(Schöberl et al., 2018).Another patient showed tau deposition primarily in the hippocampus as well as inflammation-related changes, such as lymphocyte infiltration and microglia activation (Erro et al., 2019).Interestingly, one case reported TDP-43 aggregation, in addition to tau deposition, in various microglial populations, which suggested the possibility of microglial-induced neuronal damage (Cagnin et al., 2017).In these patients, tauopathy was accompanied by inflammation or an abnormal immune microenvironment.Furthermore, in two patients, biopsy results showed no evidence of tau deposition (Montagna et al., 2018; Morales-Briceño et al., 2018).One of these patients had severe white matter lesions with increased macrophage and lymphocyte infiltration (Montagna et al., 2018), while the other showed infiltration of histiocytes and lymphocytes, increased numbers of microglia,microglial activation, and edema (Morales-Briceño et al., 2018).These patients had immune and inflammatory activation in the brain, but no evidence of tauopathy.Combined with the finding of increased B cell numbers in the CSF,these observations suggest that inflammation may independently dominate the disease in the early stages.These distinct pathological manifestations highlight the need for clinicians and researchers to carefully consider the correlation between autoimmunity, inflammation, and neurodegeneration in the treatment of anti-IgLON5 disease.
Anti-IgLON5 disease-related tauopathy may involve a novel neurodegenerative disease process that differs from that of traditional tauopathies.Tau isoforms and deposition sites in anti-IgLON5 disease are different from those in other traditional tauopathies, such as Alzheimer’s disease (AD), progressive supranuclear palsy, and corticobasal degeneration (Arendt et al., 2016).The tau isoforms identified in anti-IgLON5 disease to date include three-repeat(3R) and four-repeat (4R) isoforms (Gelpi et al., 2016).These are mainly found in neurons, and only seldom in glia and white matter (Gelpi et al.,2016).Moreover, the complex pathology of this disorder makes it difficult to classify it as a traditional tauopathy.More work is needed to determine the connection between tau and anti-IgLON5 antibodies.The neuropathological findings since 2014 are summarized in Table 1.

Table 1 |Neuropathological findings from patients with anti-IgLON5 disease since 2014
Anti-IgLON5 Antibody as a ‘Culprit’ Antibody:the Link between Neuroimmunology and Neurodegeneration
Because anti-IgLON5 disease was only recently described, research relating to this condition is still limited.However, important insights and information can still be obtained from related studies.
In vitro experiments
Sabater et al.(2014) detected IgLON5 antibodies and tau deposition in patients with anti-IgLON5 disease.They further demonstrated that the IgG1 subtype, which targets the Ig-like domain 2 of IgLON5, induced the time-dependent, irreversible internalization of IgLON5 in rat hippocampal neurons (Sabater et al., 2016).Two studies have provided evidence for neurodegenerationin vitro
.Landa et al.(2020) revealed that the IgLON5 antibody disrupted the cytoskeleton in rat hippocampal neurons, resulting in dystrophic axons and axon swelling after 3 weeks.They also discovered an increased concentration of neurofilament light chain in CSF, which is a marker of axonal damage.One clinical study reported that a correlation may exist between high serum concentrations of neurofilament light chain and the risk of death (Grüter et al., 2022).Although this study demonstrated damage to the cytoskeleton, which has a close association with tau protein (Mietelska-Porowska et al., 2014), p-tau deposition was not observed.Ryding et al.(2021) demonstrated that anti-IgLON5 antibodies induced p-tau accumulation in differentiated human neural stem cells and further reported that the proportion of p-tau-positive neurons was increased, while synaptic structure and function were disrupted.Additionally, increased neuronal death was observed after 21 days of exposure to anti-IgLON5 antibodies compared with exposure to control IgG (Ryding et al., 2021).Finally, the authors found that neurodegeneration was accompanied by a continuous reduction in IgLON5 concentrations (Ryding et al., 2021).Combined, these studies confirmed that anti-IgLON5 antibodies can directly damage nerve cells.In vivo experiments
A pilot study in mice confirmed p-tau depositionin vivo
(Alvente et al., 2022).Humanized transgenic hTau mice and C57BL/6J wild-type (WT) mice, which served as controls, were infused intracerebroventricularly with human IgLON5 antibody or control antibody for 14 days.Neuropathological examination showed p-tau deposition in the hippocampal CA4 region, mossy fibers, and posterior periependymal areas in both WT and transgenic mice.Furthermore,a longer ventilatory period during sleep and a shorter inter-lick interval during wakefulness were observed in IgLON5 antibody-treated mice with no additional differences in sleep, respiration, or motor function.These results were suggestive of an increase in airway resistance and possible behavioral stress following the infusion of the IgLON5 antibody.Ni et al.(2022a) revealed long-term cognitive impairment and anxiety-like behavior in mice infused with anti-IgLON5 antibodies.They established two models of anti-IgLON5 disease using C57BL/6 mice—stereotactic injection in the hippocampal CA1 region and ventricular cannula embedment—and noted that cognition-related neural circuits and synaptic homeostasis were both disrupted, which could explain the behavioral results.The most recent study has provided clues regarding the dual effects of the IgLON5 antibody (Ni et al., 2022a).First, the IgLON5 antibody was found to exert long-term pathogenic effectsin vivo
.The authors reported the extended binding between anti-IgLON5 antibodies from patients and the mouse brain(Ni et al., 2022a), which was consistent with the findings of Sabater et al.(2016).Three other studies also directly revealed the neuronal damage and degeneration induced by the IgLON5 antibody, thereby consolidating the linkage between the antibody and neurodegeneration.Secondly, IgLON5 antibodies may induce brain inflammation.Neuroinflammation was observedin vivo
, and included the gradual activation of microglia and astrocytes, as well as an increase in the relative mRNA expression levels of several inflammatory factors, including TGF-β, CCL5, and CXCL13 (Ni et al., 2022a).Inflammationrelated changes in the CSF and pathological findings have also been reported in several cases.These observations indicate that the IgLON5 antibody can affect neurons both directly and indirectly by inducing inflammation.Ni et al.(2022a) reported neuronal loss and morphological changes on day 30 after IgLON5 antibody injection in the presence of both antibody and inflammation.Nevertheless, the function of the IgLON5 antibody is still largely unknown, and the crucial pathways involved in how IgLON5 antibodies promote neuronal damage remain to be determined.The possible mechanisms underlying the pathophysiology of anti-IgLON5 disease based on current knowledge are depicted in Figure 2.We hypothesize that the deposition of tau protein seen in some of the patients was the result of the long-term effect of the IgLON5 antibody.
Figure 1|The crystal structure and possible configurations of IgLON5.
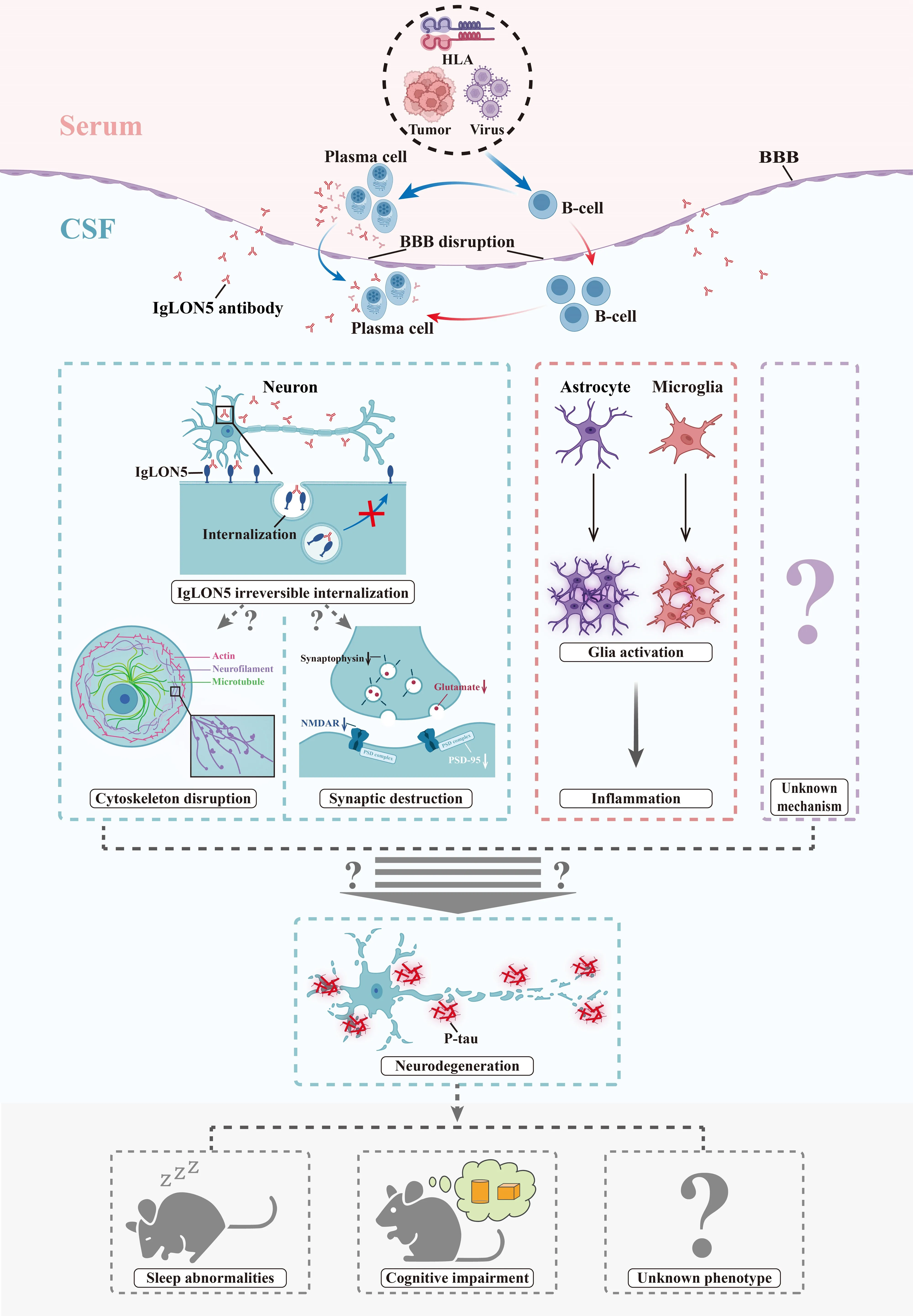
Figure 2|The possible mechanisms underlying the pathophysiology of anti-IgLON5 disease.
Perspective: Challenges and Future Directions
Anti-IgLON5 disease was only recently described; accordingly, several important questions regarding this condition remain to be answered.
First, what is the definite cause of anti-IgLON5 disease? Abnormal immunity,viral infection, tumor, and genetic susceptibility are all possible etiologies.Some patients exhibited vitiligo (Haitao et al., 2017) or renal oncocytoma(Ramanan et al., 2018) before disease onset.Also, it is known that the skin and adrenal glands express IgLON5 RNA.Meanwhile, the Epstein-Barr virus(Ni et al., 2022b) and herpes virus (Wang et al., 2022) have been detected in some patients, and either virus could induce cross-reactions.HLA-DRB1 was proposed to present sequences in the signal peptide and Ig-like domain 2 of IgLON5 to CD4T cells and induce antibody production (Gaig et al., 2019).Furthermore, some patients display fasciculation (Wenninger, 2017) and cardiac symptoms (Montojo et al., 2016).Given that IgLON5 was reported to be present in skeletal muscle and myocardium, it should also be clarified whether organs outside the central nervous system can be directly targeted.
Second, what are the differences between the IgG1 and IgG4 subtypes?Current evidence only explains the effect of internalization of the IgG1 subtype in anti-IgLON5 disease.The IgG1 antibody is bivalent and Fc-dependent, which causes cross-linking between antigens and the complement cascade in other diseases, such as anti-NMDAR autoimmune encephalitis (Hughes et al., 2010)and neuromyelitis optica spectrum disorder (Duan et al., 2019).It seems that the IgG4 subtype mainly disrupts protein-protein interactions because of the univalent nature of Fab-arm exchange, which affects signal transduction and cell adhesion (Koneczny, 2020).IgG4-mediated autoimmune diseasesare insidious and fatal (Perugino and Stone, 2020).These characteristics are highly consistent with anti-IgLON5 disease, suggesting the important role of IgG4.As both subtypes are present simultaneously in patients, it should be further clarified whether these subtypes exert dominant or synergistic effects in this disease.
Third, which pathways mediate the effects of the antibodies on neurodegeneration? As discussed above, the IgLON5 antibody acts in concert with IgLON5 to initiate the neurodegenerative process.However, the specific signaling pathways involved need to be further explored.IgLON5 antibodies may exist in the body for extended periods due to genetic abnormality,thereby exerting long-term effects on neurons.In addition, inflammation has been observedin vivo
and may be another cause of neuronal damage.Appropriate animal models must be established, such as those relating to active immunity, to better explore the natural processes of the disease.Finally, how can the diagnosis and treatment of anti-IgLON5 disease be improved? Given the complex phenotypes and potentially poor long-term outcomes, early diagnosis and treatment are needed to improve patient survival and prognosis.As the IgLON5 antibody may cause irreversible damage to neurons, exploring new strategies in addition to traditional immunotherapy, such as small-molecule targeted therapy (requires further study of antibody structure), as well as developing neuroprotective therapy,will be important for the future treatment of this disease.
Author contributions:
YZHZ, YN and YNG were responsible for the literature review and writing of the manuscript.DDS, LH, DY, HYM, QMZ, JH, and SC helped with editing and modifying the manuscript.SC designed this manuscript.All the authors approved the final version of the manuscript.
Conflicts of interest:
There are no conflicts of interest.
Availability of data and materials:
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Open access statement:
This is an open access journal, and articles are distributed under the terms of the Creative Commons AttributionNonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Additional file:
Clinical research of anti-IgLON5 disease from 2014 to 2022.
- 中国神经再生研究(英文版)的其它文章
- Patient-specific monocyte-derived microglia as a screening tool for neurodegenerative diseases
- Molecular hallmarks of long non-coding RNAs in aging and its significant effect on aging-associated diseases
- Inflammation in diabetic retinopathy: possible roles in pathogenesis and potential implications for therapy
- Targeting the nitric oxide/cGMP signaling pathway to treat chronic pain
- Neurosteroids as stress modulators and neurotherapeutics: lessons from the retina
- Myelinosome organelles in pathological retinas:ubiquitous presence and dual role in ocular proteostasis maintenance